

Phase II/III trial of a pre-transplant farnesyl transferase inhibitor in juvenile myelomonocytic leukemia: a report from the Children's Oncology Group
- PMID: 25704135
- PMCID: PMC4339233
- DOI: 10.1002/pbc.25342
Phase II/III trial of a pre-transplant farnesyl transferase inhibitor in juvenile myelomonocytic leukemia: a report from the Children's Oncology Group
Abstract
Background: Juvenile myelomonocytic leukemia (JMML) is not durably responsive to chemotherapy, and approximately 50% of patients relapse after hematopoietic stem cell transplant (HSCT). Here we report the activity and acute toxicity of the farnesyl transferase inhibitor tipifarnib, the response rate to 13-cis retinoic acid (CRA) in combination with cytoreductive chemotherapy, and survival following HSCT in children with JMML.
Procedure: Eighty-five patients with newly diagnosed JMML were enrolled on AAML0122 between 2001 and 2006. Forty-seven consented to receive tipifarnib in a phase II window before proceeding to a phase III trial of CRA in combination with fludarabine and cytarabine followed by HSCT and maintenance CRA. Thirty-eight patients enrolled only in the phase III trial.
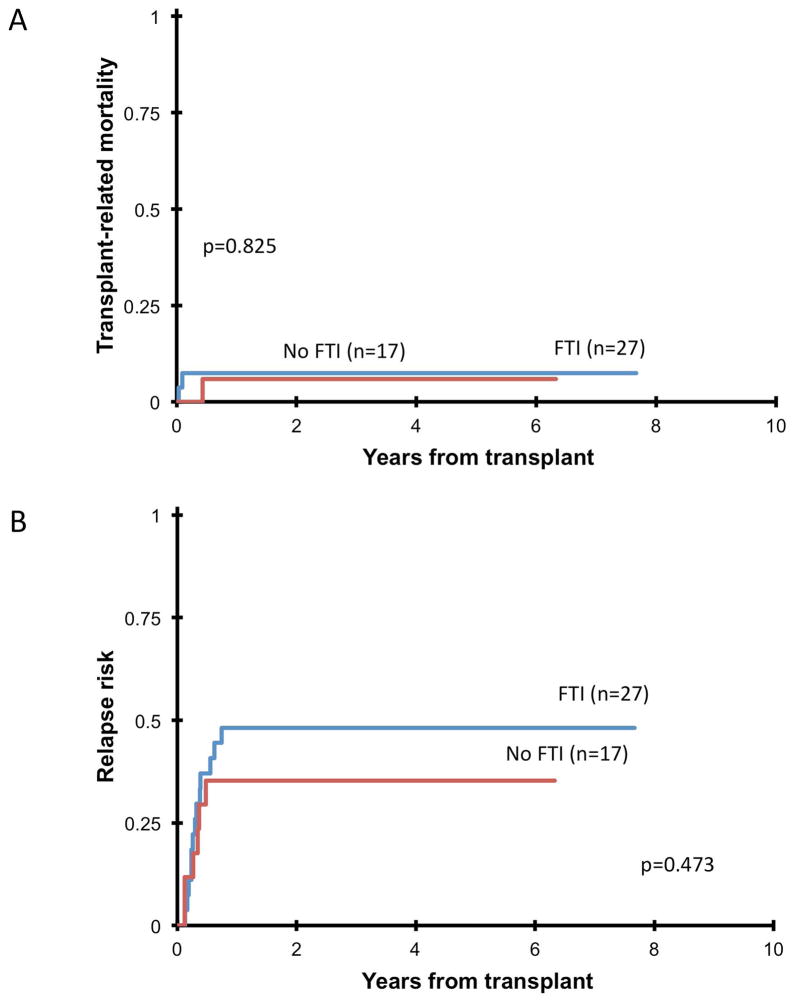
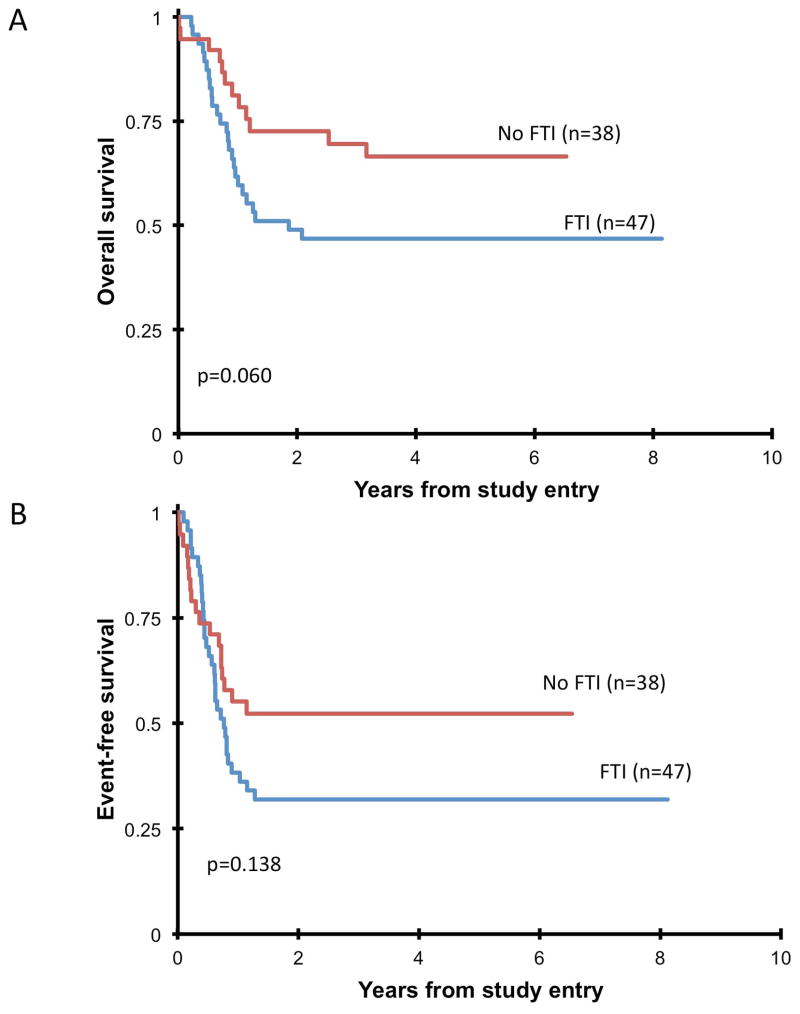
Results: Overall response rate was 51% after tipifarnib and 68% after fludarabine/cytarabine/CRA. Tipifarnib did not increase pre-transplant toxicities. Forty-six percent of the 44 patients who received protocol compliant HSCT relapsed. Five-year overall survival was 55 ± 11% and event-free survival was 41 ± 11%, with no significant difference between patients who did or did not receive tipifarnib.
Conclusions: Administration of tipifarnib in the window setting followed by HSCT in patients with newly diagnosed JMML was safe and yielded a 51% initial response rate as a single agent, but failed to reduce relapse rates or improve long-term overall survival.
Keywords: 13-cis retinoic acid; farnesyl transferase inhibitor; hematopoietic stem cell transplant; juvenile myelomonocytic leukemia; tipifarnib.
© 2014 Wiley Periodicals, Inc.
Conflict of interest statement
Peter D. Emanuel has research funding from Johnson and Johnson. The remaining authors declare no conflict of interest.
Figures
References
-
- Busque L, Gilliland DG, Prchal JT, et al. Clonality in juvenile chronic myelogenous leukemia. Blood. 1995;85:21–30. - PubMed
-
- Niemeyer CM, Arico M, Basso G, et al. Chronic myelomonocytic leukemia in childhood: a retrospective analysis of 110 cases. European Working Group on Myelodysplastic Syndromes in Childhood (EWOG-MDS) Blood. 1997;89:3534–3543. - PubMed
-
- Emanuel PD, Bates LJ, Castleberry RP, et al. Selective hypersensitivity to granulocyte-macrophage colony-stimulating factor by juvenile chronic myeloid leukemia hematopoietic progenitors. Blood. 1991;77:925–929. - PubMed
-
- Emanuel PD. Juvenile myelomonocytic leukemia. Curr Hematol Rep. 2004;3:203–209. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
