

Management of hypertension in CKD: beyond the guidelines
- PMID: 25704348
- PMCID: PMC4445132
- DOI: 10.1053/j.ackd.2014.12.001
Management of hypertension in CKD: beyond the guidelines
Abstract
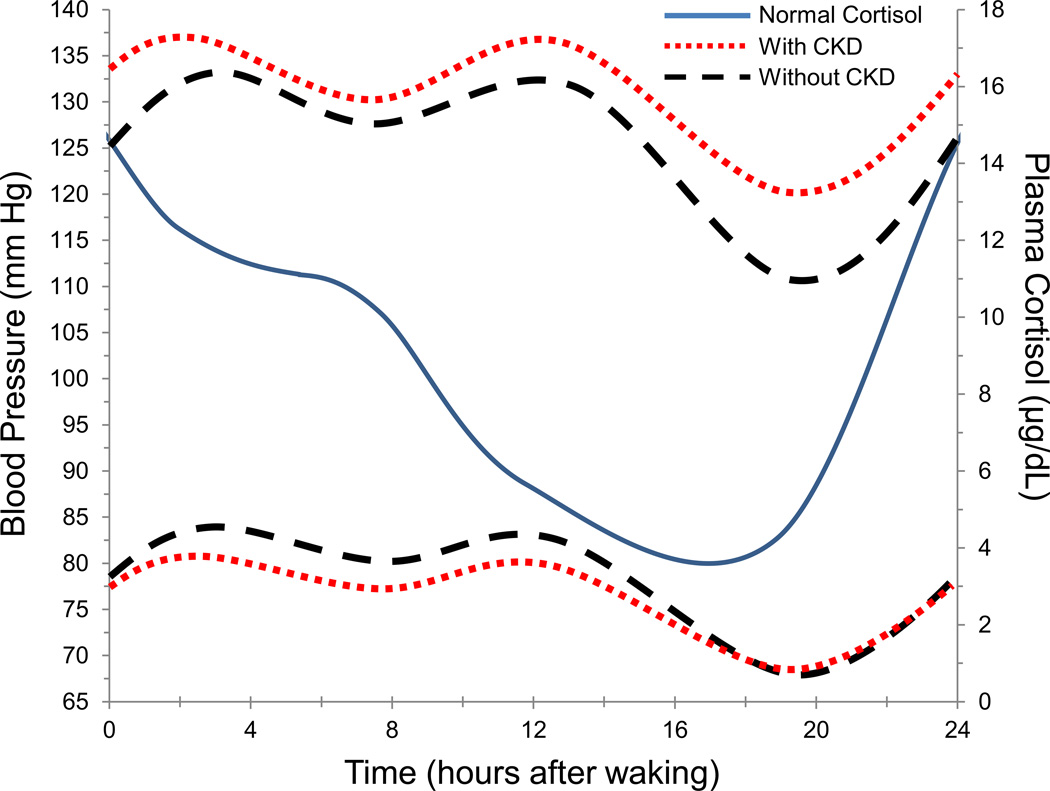
Hypertension (HTN) and CKD are closely associated with an intermingled cause and effect relationship. Blood pressure (BP) typically rises with declines in kidney function, and sustained elevations in BP hasten progression of kidney disease. This review addresses current management issues in HTN in patients with CKD including altered circadian rhythm of BP, timing of antihypertensive medication dosing, BP targets, diagnostic challenges in evaluating secondary forms of HTN, and the role of salt restriction in CKD. HTN in patients with CKD is often accompanied by a decrease in the kidney's ability to remove salt. Addressing this salt sensitivity is critical for the management of HTN in CKD. In addition to the well-established use of an ACEI or angiotensin receptor blocker, dietary salt restriction and appropriate diuretic therapy make up the mainstay of HTN treatment in patients with CKD. Bedtime dosing of antihypertensive medications can restore nocturnal dips in BP, and future clinical practice guidelines may recommend bedtime dosing of 1 or more antihypertensive medications in patients with CKD.
Keywords: Blood pressure; CKD; Hypertension; Resistant; Salt.
Copyright © 2015 National Kidney Foundation, Inc. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Bakris GL, Williams M, Dworkin L, et al. Preserving renal function in adults with hypertension and diabetes: a consensus approach. National Kidney Foundation Hypertension and Diabetes Executive Committees Working Group. Am J Kidney Dis. 2000;36(3):646–661. - PubMed
-
- Egan BM, Zhao Y, Axon RN. US trends in prevalence, awareness, treatment, and control of hypertension, 1988–2008. JAMA. 2010;303(20):2043–2050. - PubMed
-
- Cai G, Zheng Y, Sun X, Chen X. Prevalence, awareness, treatment, and control of hypertension in elderly adults with chronic kidney disease: results from the survey of Prevalence, Awareness, and Treatment Rates in Chronic Kidney Disease Patients With Hypertension in China. J Am Geriatr Soc. 2013;61(12):2160–2167. - PubMed
-
- Tozawa M, Iseki K, Iseki C, Kinjo K, Ikemiya Y, Takishita S. Blood pressure predicts risk of developing end-stage renal disease in men and women. Hypertension. 2003;41(6):1341–1345. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
