

F-18 fluoromisonidazole for imaging tumor hypoxia: imaging the microenvironment for personalized cancer therapy
- PMID: 25704387
- PMCID: PMC4339212
- DOI: 10.1053/j.semnuclmed.2014.10.006
F-18 fluoromisonidazole for imaging tumor hypoxia: imaging the microenvironment for personalized cancer therapy
Abstract
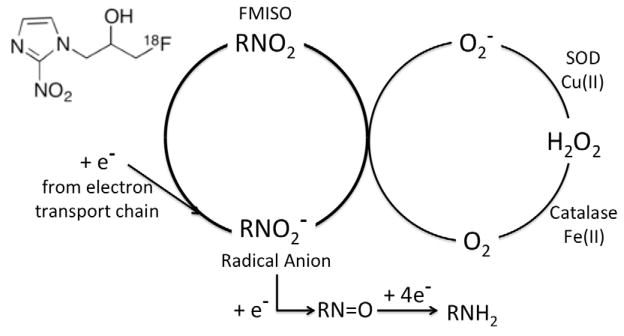
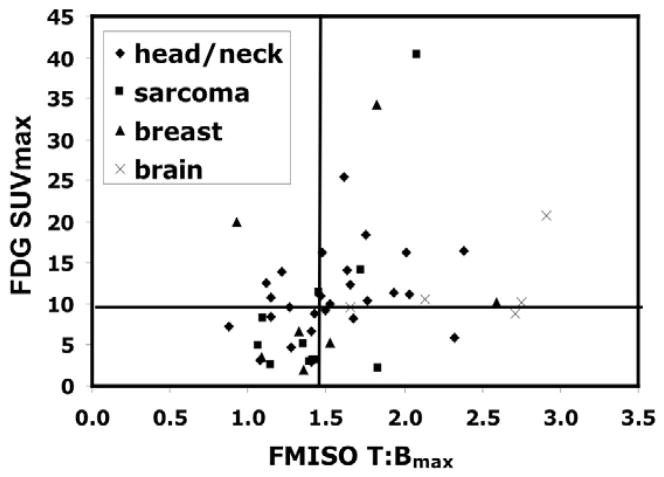
Hypoxia in solid tumors is one of the seminal mechanisms for developing aggressive trait and treatment resistance in solid tumors. This evolutionarily conserved biological mechanism along with derepression of cellular functions in cancer, although resulting in many challenges, provide us with opportunities to use these adversities to our advantage. Our ability to use molecular imaging to characterize therapeutic targets such as hypoxia and apply this information for therapeutic interventions is growing rapidly. Evaluation of hypoxia and its biological ramifications to effectively plan appropriate therapy that can overcome the cure-limiting effects of hypoxia provides an objective means for treatment selection and planning. Fluoromisonidazole (FMISO) continues to be the lead radiopharmaceutical in PET imaging for the evaluation, prognostication, and quantification of tumor hypoxia, one of the key elements of the tumor microenvironment. FMISO is less confounded by blood flow, and although the images have less contrast than FDG-PET, its uptake after 2 hours is an accurate reflection of inadequate regional oxygen partial pressure at the time of radiopharmaceutical administration. By virtue of extensive clinical utilization, FMISO remains the lead candidate for imaging and quantifying hypoxia. The past decade has seen significant technological advances in investigating hypoxia imaging in radiation treatment planning and in providing us with the ability to individualize radiation delivery and target volume coverage. The presence of widespread hypoxia in the tumor can be effectively targeted with a systemic hypoxic cell cytotoxin or other agents that are more effective with diminished oxygen partial pressure, either alone or in combination. Molecular imaging in general and hypoxia imaging in particular will likely become an important in vivo imaging biomarker of the future, complementing the traditional direct tissue sampling methods by providing a snap shot of a primary tumor and metastatic disease and in following treatment response and will serve as adjuncts to personalized therapy.
Published by Elsevier Inc.
Figures



References
-
- Awada A, Aftimos PG. Targeted therapies of solid cancers: new options, new challenges. Curr Opin Oncol. 2013;25(3):296–304. - PubMed
-
- Thomlinson RH. Tumour anoxia and the response to radiation. Sci Basis Med Annu Rev. 1965:74–90. - PubMed
-
- Hanahan D, Weinberg RA. Hallmarks of cancer: the next generation. Cell. 2011;144(5):646–74. - PubMed
-
- Wijsman R, Kaanders JH, Oyen WJ, Bussink J. Hypoxia and tumor metabolism in radiation oncology: targets visualized by positron emission tomography. Q J Nucl Med Mol Imaging. 2013;57(3):244–56. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
