

Dynamic contrast-enhanced MRI evaluates the early response of human head and neck tumor xenografts following anti-EMMPRIN therapy with cisplatin or irradiation
- PMID: 25704985
- PMCID: PMC4545484
- DOI: 10.1002/jmri.24871
Dynamic contrast-enhanced MRI evaluates the early response of human head and neck tumor xenografts following anti-EMMPRIN therapy with cisplatin or irradiation
Abstract
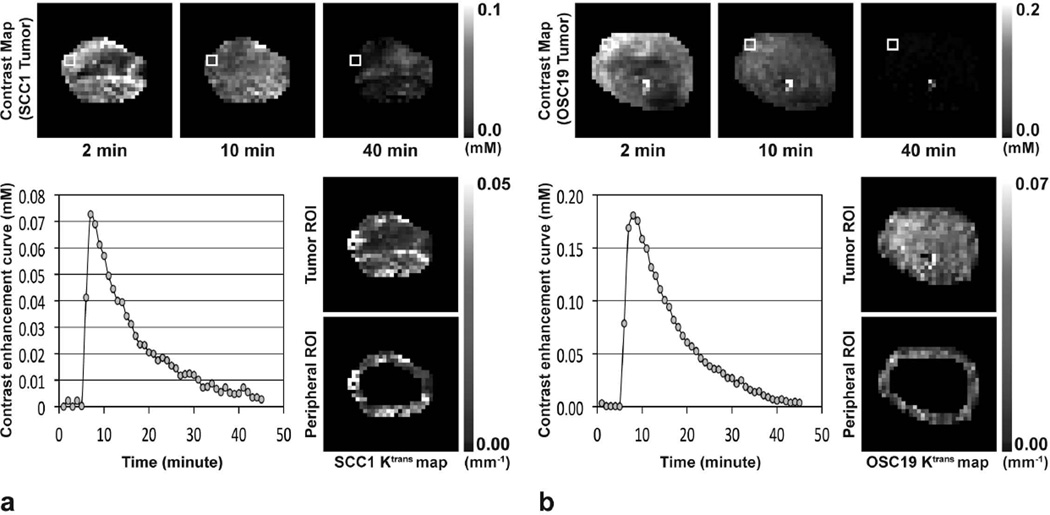
Purpose: To assess the early therapeutic effects of anti-EMMPRIN (extracellular matrix metalloprotease inducer) antibody with/without cisplatin or X-ray radiation in head and neck cancer mouse models using dynamic contrast-enhanced magnetic resonance imaging (DCE-MRI).
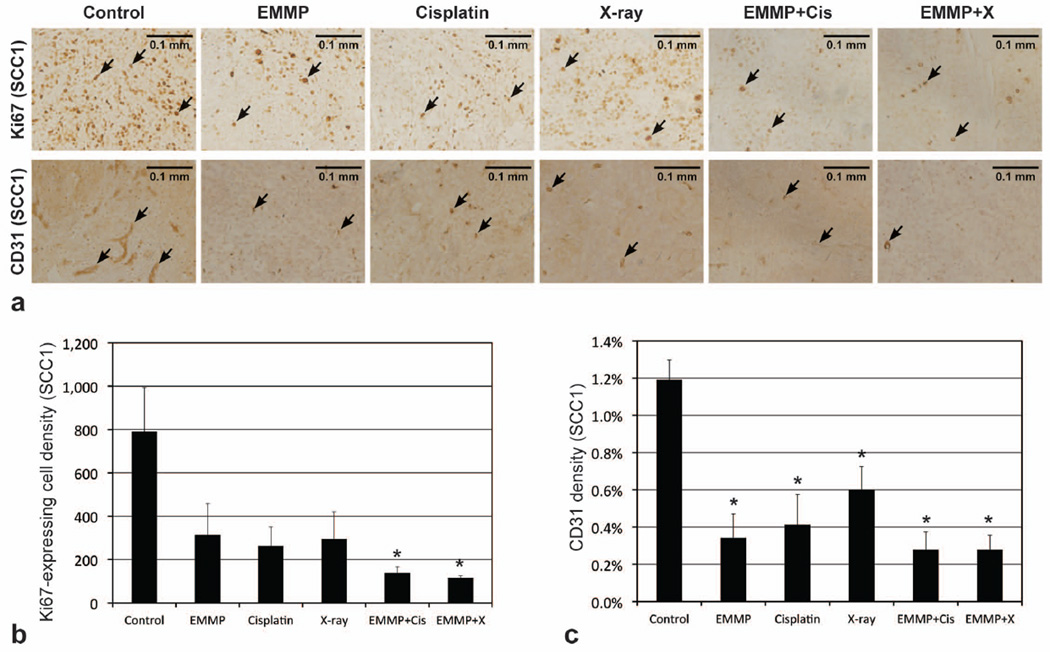
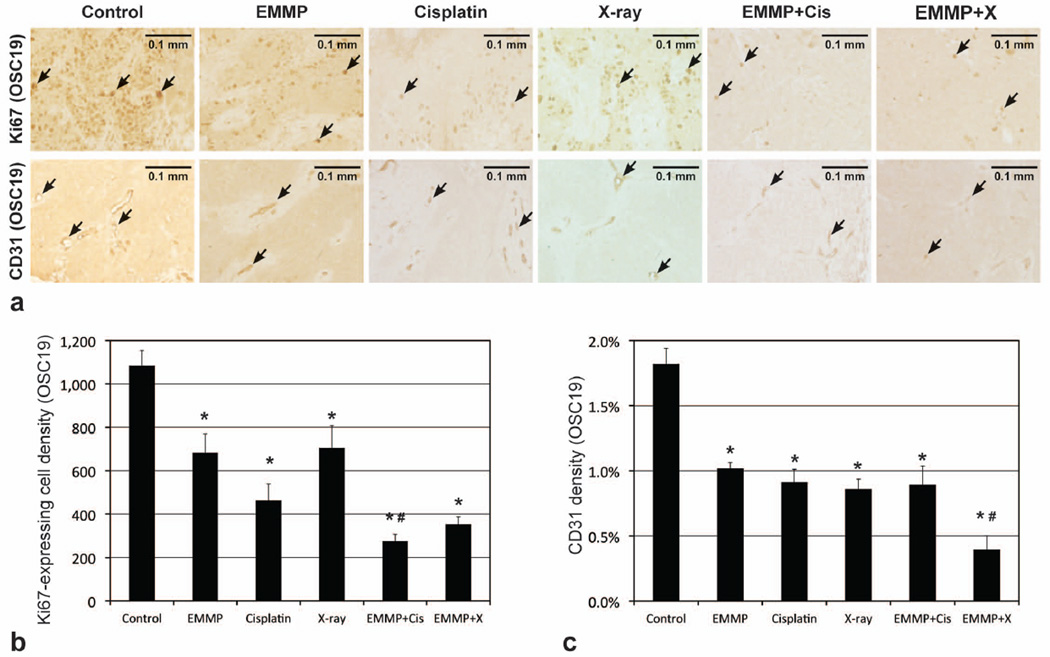
Materials and methods: Mice bearing SCC1 (or OSC19) tumor xenografts were treated with anti-EMMPRIN antibody, radiation, cisplatin, or anti-EMMPRIN antibody plus cisplatin (or radiation) for a week (n = 4-5 per group). DCE-MRI was carried out on a 9.4T small animal MR scanner on days 0, 3, and 7, and K(trans) values were averaged in a 0.5-mm-thick peripheral tumor region. Ki67 and CD31 staining were implemented for all tumors after imaging.
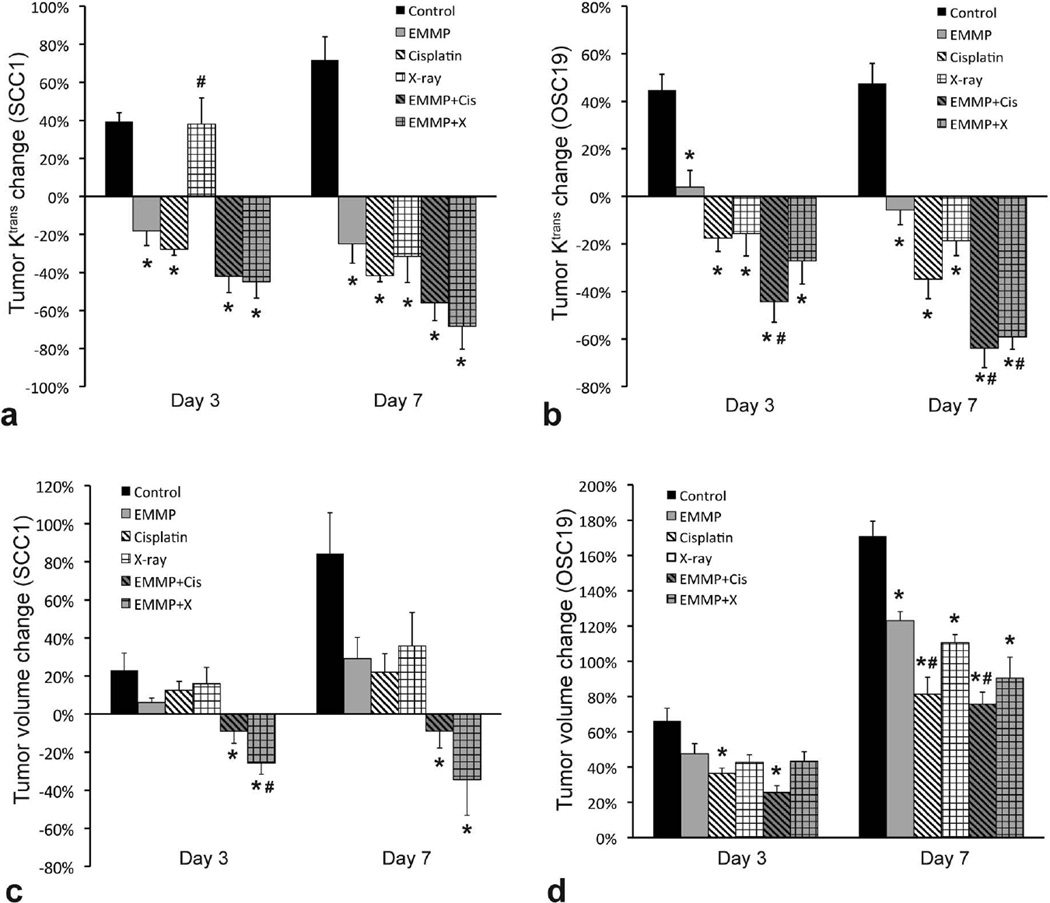
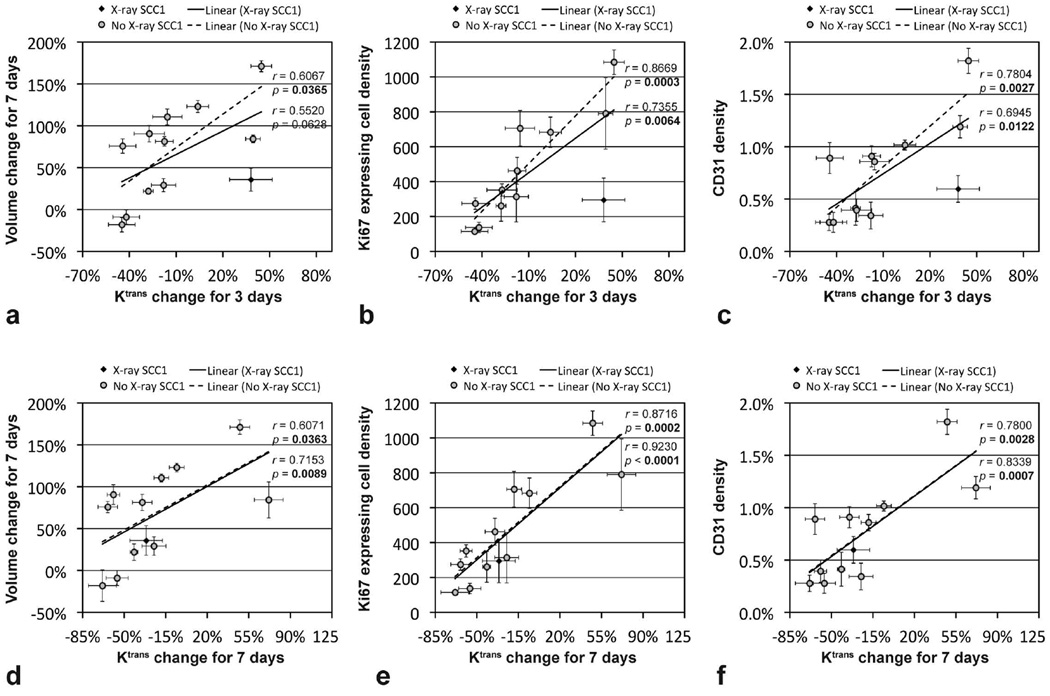
Results: The K(trans) changes of SCC1 and OSC19 tumors treated with anti-EMMPRIN antibody for 3 days were -18 ± 8% and 4 ± 7%, respectively, which were significantly lower than those of control groups (39 ± 5% and 45 ± 7%; P = 0.0025 and 0.0220, respectively). When cisplatin was added, those were -42 ± 9% and -44 ± 9%, respectively, and with radiation, -45 ± 9% and -27 ± 10%, respectively, which were also significantly lower than those of control groups (P < 0.0001 for all four comparisons). In the eight groups untreated (served as control) or treated with anti-EMMPRIN antibody with/without cisplatin or radiation, the mean K(trans) change for 3 days was significantly correlated with the mean tumor volume change for 7 days (r = 0.74, P = 0.0346), Ki67-expressing cell density (r = 0.96, P = 0.0001), and CD31 density (r = 0.84, P = 0.0084).
Conclusion: DCE-MRI might be utilized to assess the early therapeutic effects of anti-EMMPRIN antibody with/without chemotherapy or radiotherapy in head and neck cancer.
Keywords: DCE-MRI; anti-EMMPRIN antibody; cisplatin; head and neck cancer; radiotherapy.
© 2015 Wiley Periodicals, Inc.
Figures
Similar articles
-
Dynamic contrast-enhanced MRI in head-and-neck cancer: the impact of region of interest selection on the intra- and interpatient variability of pharmacokinetic parameters.Int J Radiat Oncol Biol Phys. 2012 Mar 1;82(3):e345-50. doi: 10.1016/j.ijrobp.2011.05.059. Epub 2011 Oct 8. Int J Radiat Oncol Biol Phys. 2012. PMID: 21985945 Clinical Trial.
-
Anti-EMMPRIN monoclonal antibody as a novel agent for therapy of head and neck cancer.Clin Cancer Res. 2009 Jun 15;15(12):4058-65. doi: 10.1158/1078-0432.CCR-09-0212. Epub 2009 Jun 9. Clin Cancer Res. 2009. PMID: 19509148 Free PMC article.
-
Assessment of early therapeutic response to sorafenib in renal cell carcinoma xenografts by dynamic contrast-enhanced and diffusion-weighted MR imaging.Br J Radiol. 2015 Sep;88(1053):20150163. doi: 10.1259/bjr.20150163. Epub 2015 Jul 2. Br J Radiol. 2015. PMID: 26133222 Free PMC article.
-
Definitive chemoradiotherapy for squamous head and neck cancer: cisplatin versus carboplatin? A meta-analysis.Future Oncol. 2016 Dec;12(23):2755-2764. doi: 10.2217/fon-2016-0068. Epub 2016 Aug 23. Future Oncol. 2016. PMID: 27549331 Review.
-
Dynamic Contrast-Enhanced MR Imaging in Head and Neck Cancer.Magn Reson Imaging Clin N Am. 2018 Feb;26(1):135-149. doi: 10.1016/j.mric.2017.08.008. Epub 2017 Oct 21. Magn Reson Imaging Clin N Am. 2018. PMID: 29128001 Review.
Cited by
-
Functional MRI for the prediction of treatment response in head and neck squamous cell carcinoma: potential and limitations.Cancer Imaging. 2016 Aug 19;16(1):23. doi: 10.1186/s40644-016-0080-6. Cancer Imaging. 2016. PMID: 27542718 Free PMC article. Review.
-
Extracellular vesicles originating from glioblastoma cells increase metalloproteinase release by astrocytes: the role of CD147 (EMMPRIN) and ionizing radiation.Cell Commun Signal. 2020 Feb 7;18(1):21. doi: 10.1186/s12964-019-0494-4. Cell Commun Signal. 2020. PMID: 32033611 Free PMC article.
-
Dynamic Contrast-Enhanced MR Imaging of Nonenhancing T2 High-Signal-Intensity Lesions in Baseline and Posttreatment Glioblastoma: Temporal Change and Prognostic Value.AJNR Am J Neuroradiol. 2020 Jan;41(1):49-56. doi: 10.3174/ajnr.A6323. Epub 2019 Dec 5. AJNR Am J Neuroradiol. 2020. PMID: 31806595 Free PMC article.
References
-
- Siegel R, Ma J, Zou Z, Jemal A. Cancer statistics, 2014. CA: a cancer journal for clinicians. 2014;64:9–29. - PubMed
-
- Brana I, Siu LL. Locally advanced head and neck squamous cell cancer: treatment choice based on risk factors and optimizing drug prescription. Ann Oncol. 2012;23(Suppl 10):x178–x185. - PubMed
-
- Rousseau A, Badoual C. Head and Neck: Squamous cell carcinoma: an overview. Atlas Genet Cytogenet Oncol Haematol. 2012;16:145–155.
-
- Casiglia J, Woo SB. A comprehensive review of oral cancer. Gen Dent. 2001;49:72–82. - PubMed
-
- Faratian D, Clyde RG, Crawford JW, Harrison DJ. Systems pathology--taking molecular pathology into a new dimension. Nat Rev Clin Oncol. 2009;6:455–464. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
