

Treatment of thoracolumbar fracture
- PMID: 25705347
- PMCID: PMC4330209
- DOI: 10.4184/asj.2015.9.1.133
Treatment of thoracolumbar fracture
Abstract
The most common fractures of the spine are associated with the thoracolumbar junction. The goals of treatment of thoracolumbar fracture are leading to early mobilization and rehabilitation by restoring mechanical stability of fracture and inducing neurologic recovery, thereby enabling patients to return to the workplace. However, it is still debatable about the treatment methods. Neurologic injury should be identified by thorough physical examination for motor and sensory nerve system in order to determine the appropriate treatment. The mechanical stability of fracture also should be evaluated by plain radiographs and computed tomography. In some cases, magnetic resonance imaging is required to evaluate soft tissue injury involving neurologic structure or posterior ligament complex. Based on these physical examinations and imaging studies, fracture stability is evaluated and it is determined whether to use the conservative or operative treatment. The development of instruments have led to more interests on the operative treatment which saves mobile segments without fusion and on instrumentation through minimal invasive approach in recent years. It is still controversial for the use of these treatments because there have not been verified evidences yet. However, the morbidity of patients can be decreased and good clinical and radiologic outcomes can be achieved if the recent operative treatments are used carefully considering the fracture pattern and the injury severity.
Keywords: Fracture; Minimally invasive surgery; Thoracolumbar spine; Treatment.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported
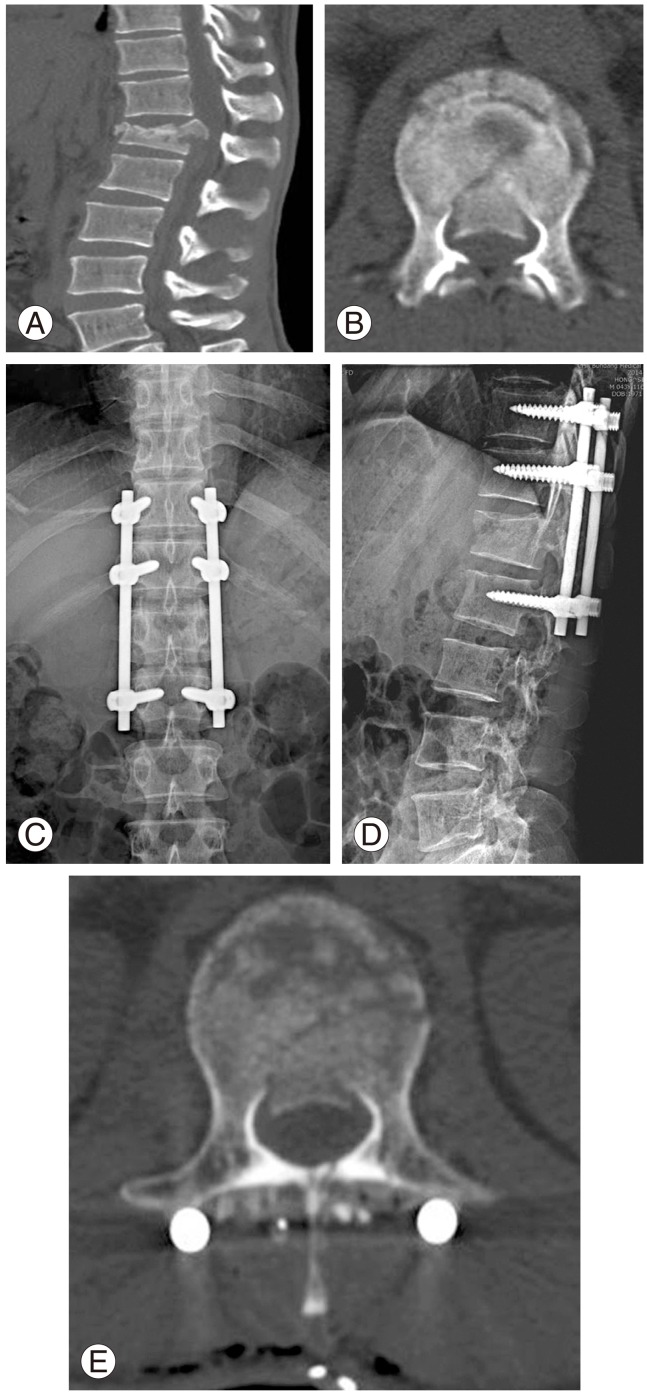
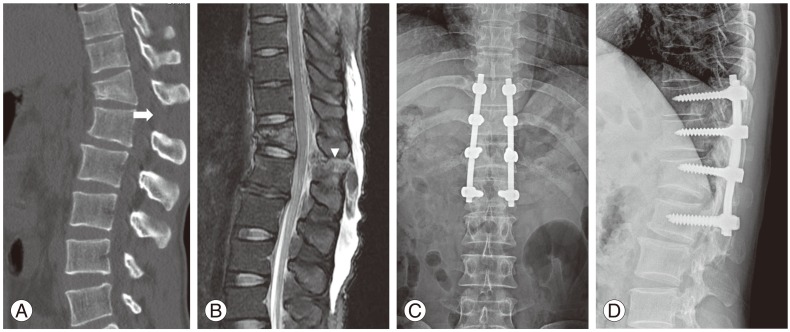
Figures

References
-
- DeWald RL. Burst fractures of the thoracic and lumbar spine. Clin Orthop Relat Res. 1984;(189):150–161. - PubMed
-
- Gertzbein SD. Scoliosis Research Society. Multicenter spine fracture study. Spine (Phila Pa 1976) 1992;17:528–540. - PubMed
-
- Rockwood CA, Green DP, Bucholz RW. Rockwood and Green's fractures in adults. Philadelphia: Lippincott Williams & Wilkins; 2006.
-
- Kim DH, Silber JS, Albert TJ. Osteoporotic vertebral compression fractures. Instr Course Lect. 2003;52:541–550. - PubMed
-
- Hsu JM, Joseph T, Ellis AM. Thoracolumbar fracture in blunt trauma patients: guidelines for diagnosis and imaging. Injury. 2003;34:426–433. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
