

Among Ectasia Patients with Coexisting Coronary Artery Disease, TIMI Frame Count Correlates with Ectasia Size and Markis Type IV Is the Commonest
- PMID: 25705544
- PMCID: PMC4332750
- DOI: 10.1155/2015/282170
Among Ectasia Patients with Coexisting Coronary Artery Disease, TIMI Frame Count Correlates with Ectasia Size and Markis Type IV Is the Commonest
Abstract
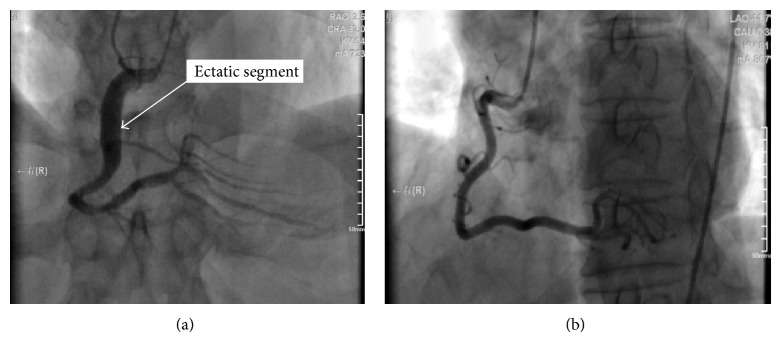
Background. Coronary artery ectasia (CAE) occurs in 0.3 to 5.3% of patients undergoing coronary angiography. TIMI frame count (TFC) is an index of coronary flow that correlates with flow velocity. In ectasia patients, there is delayed coronary flow with increased TFC. Methods. We evaluated angiograms of 789 patients for presence of CAE, coronary artery disease (CAD), and Markis type of CAE. We measured ectasia size and length and their correlation with TFC in ectatic right coronary arteries (RCA) of patients with CAE and CAD. Results. 30 patients had CAE (3.8%). Of these 16.7% had isolated CAE, while 83.87% had CAE and CAD. Among CAE and CAD patients, the RCA was most involved (70.4%), and Markis type IV CAE was the commonest (64%). In isolated CAE, the RCA, LAD, and LCx were equally involved (33.3%). Patients with CAE and CAD had significantly higher TFC compared to controls, P = 0.035. There was a positive correlation of moderate strength, between ectasia size and TFC, r(17) = 0.598, P = 0.007. Ectasia length was not significantly correlated with TFC, rho (17) = 0.334, P = 0.163. Conclusion. Among patients undergoing angiography, CAE has a prevalence of 3.8% and Markis type IV is the commonest. Larger ectasias are associated with slower coronary flow.
Figures
Similar articles
-
Effects of co-existence of coronary stenosis and the extent of coronary ectasia on the TIMI frame count in patients with coronary artery ectasia.Int Heart J. 2005 Mar;46(2):211-8. doi: 10.1536/ihj.46.211. Int Heart J. 2005. PMID: 15876805
-
Coronary flow evaluation by TIMI frame count and magnetic resonance flow velocity in patients with coronary artery ectasia.J Cardiovasc Magn Reson. 2005;7(3):545-50. doi: 10.1081/jcmr-200060641. J Cardiovasc Magn Reson. 2005. PMID: 15959966
-
Clinical and angiographic characteristics of patients with coronary artery ectasia.Int J Cardiol. 2013 Aug 20;167(4):1536-41. doi: 10.1016/j.ijcard.2012.04.098. Epub 2012 May 8. Int J Cardiol. 2013. PMID: 22572634
-
Ratio of Serum Aspartate to Alanine Aminotransferase as a Marker of Isolated Coronary Artery Ectasia and its Severity.Heart Int. 2020 Jul 31;14(1):43-48. doi: 10.17925/HI.2020.14.1.43. eCollection 2020. Heart Int. 2020. PMID: 36277666 Free PMC article. Review.
-
Treatment and Outcome of Patients With Coronary Artery Ectasia: Current Evidence and Novel Opportunities for an Old Dilemma.Front Cardiovasc Med. 2022 Feb 4;8:805727. doi: 10.3389/fcvm.2021.805727. eCollection 2021. Front Cardiovasc Med. 2022. PMID: 35187112 Free PMC article. Review.
Cited by
-
Is Coronary Artery Ectasia a Progressive Disease? A Self-Controlled Retrospective Cohort Study.Front Cardiovasc Med. 2021 Dec 6;8:774597. doi: 10.3389/fcvm.2021.774597. eCollection 2021. Front Cardiovasc Med. 2021. PMID: 34938789 Free PMC article.
-
Role of gender in types and frequency of coronary artery aneurysm and ectasia.Medicine (Baltimore). 2016 Aug;95(31):e4395. doi: 10.1097/MD.0000000000004395. Medicine (Baltimore). 2016. PMID: 27495054 Free PMC article.
-
Underlying factors relating to acute myocardial infarction for coronary artery ectasia patients.Medicine (Baltimore). 2020 Sep 4;99(36):e21983. doi: 10.1097/MD.0000000000021983. Medicine (Baltimore). 2020. PMID: 32899042 Free PMC article.
References
-
- Sultana R., Sultana N., Ishaq M., Samad A. The prevalence and clinical profile of angiographic coronary ectasia. Journal of the Pakistan Medical Association. 2011;61(4):372–375. - PubMed
-
- Pinar Bermúdez E., López Palop R., Lozano Martínez-Luengas I., et al. Coronary ectasia: prevalence, and clinical and angiographic characteristics. Revista Española de Cardiologia. 2003;56(5):473–479. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous