Outcome and graft patency in coronary artery bypass grafting with coronary endarterectomy
- PMID: 25705593
- PMCID: PMC4333844
- DOI: 10.5090/kjtcs.2015.48.1.13
Outcome and graft patency in coronary artery bypass grafting with coronary endarterectomy
Abstract
Background: Controversy persists regarding the use of coronary endarterectomy (CE) in patients with severe coronary artery disease. We compared the comorbidities and perioperative characteristics of patients undergoing coronary artery bypass grafting (CABG) with and without CE.
Methods: This study was performed in two private hospitals in Shiraz, Iran from May 2010 to December 2011 on 967 patients who underwent CABG without CE and 84 patients who underwent CABG with CE (the CE+ group). After follow-up at 9.66±3.65 months post-surgery, 28 patients from the CE+ group underwent angiography to evaluate the patency of grafts and native coronary vessels.
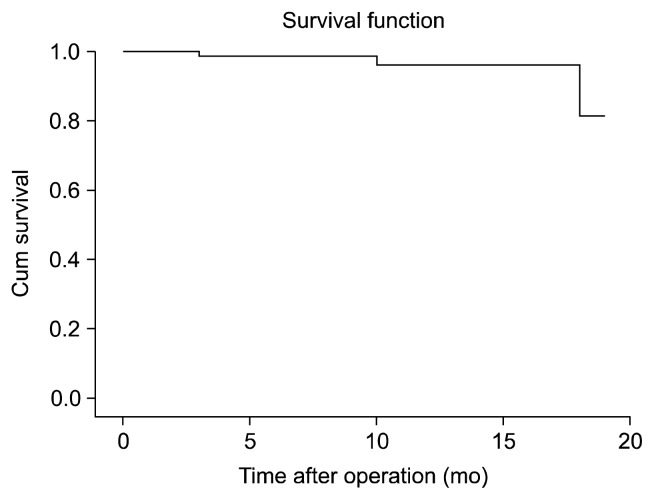
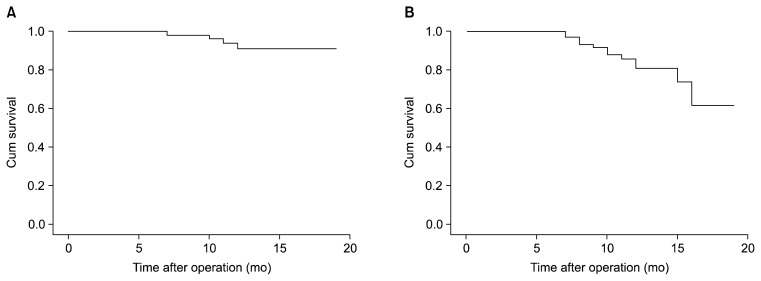
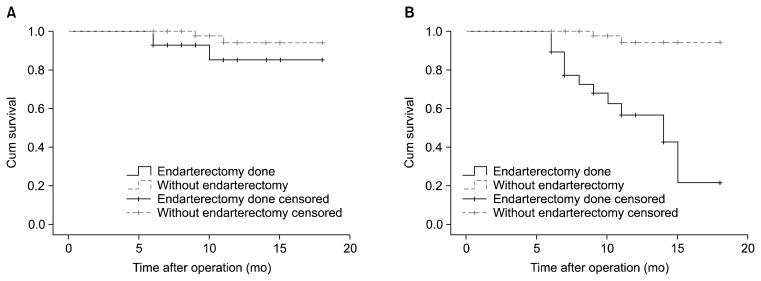
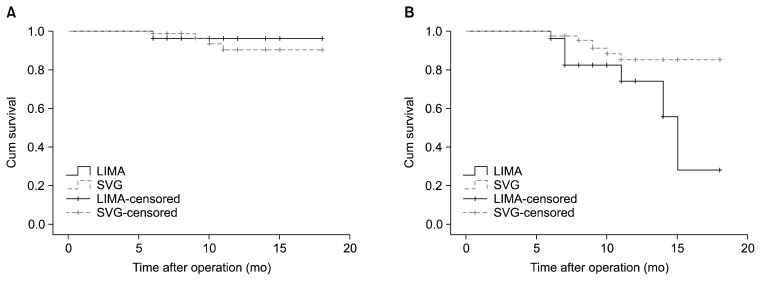
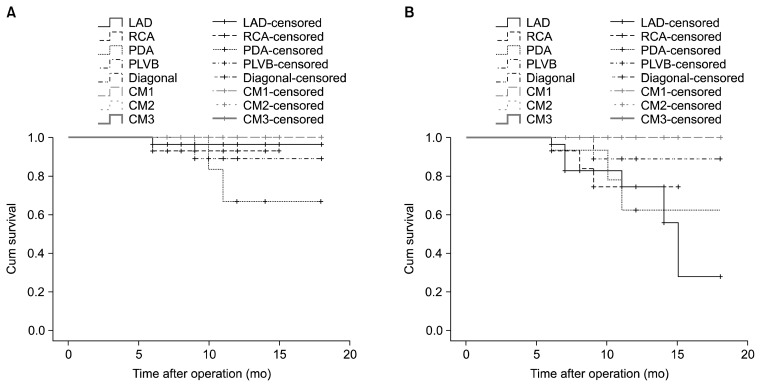
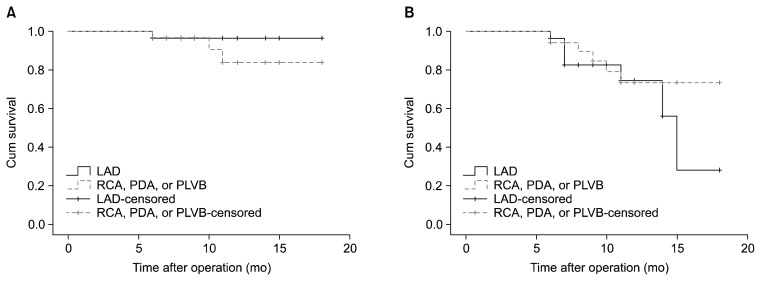
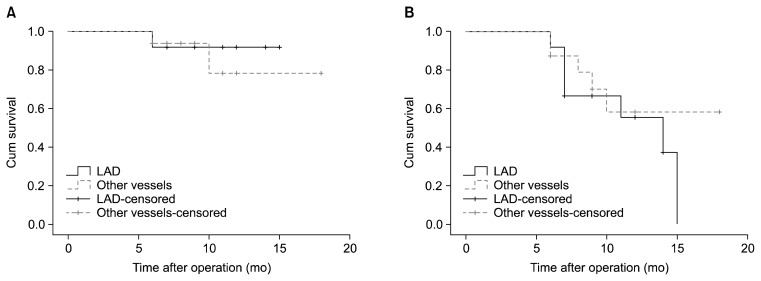
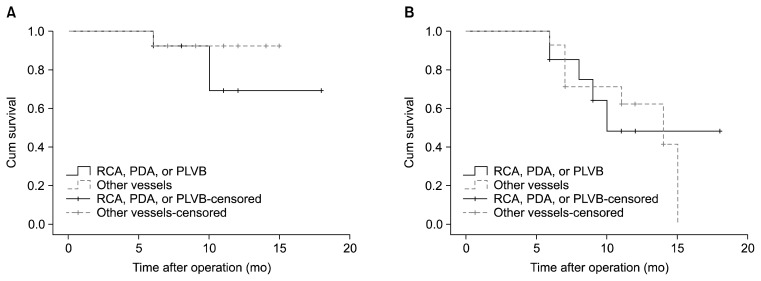
Results: Patients in the CE+ group had a more prevalent history of diabetes (48% vs. 36%) and number of diseased vessels (2.88±0.39 vs. 2.70±0.85). The overall hospital mortality was 1.8%, and no significant difference was observed between the two groups. In the 28 patients who underwent reangiography, 113 vessels were bypassed and 29 endarterectomies were performed, mostly on the left anterior descending artery (12 endarterectomies) and the right coronary artery (8 endarterectomies). In the endarterectomized vessels, a 66% patency rate was found in both the grafts and the native vessels. The native coronary vessels were more likely to be patent when the left internal mammary artery was used as a conduit than when a saphenous vein bypass graft was used.
Conclusion: The lack of a significant difference in postoperative complications in patients who underwent CABG with or without CE may indicate that CE does not expose patients to a higher risk of complications. Since most of the endarterectomized vessels were shown to be patent during the follow-up period, we propose that endarterectomy is a viable option for patients with severely diseased vessels.
Keywords: Comorbidity; Coronary artery bypass surgery; Coronary endarterectomy.
Figures
Similar articles
-
[The early and midterm results of coronary endarterectomy combined with coronary artery bypass grafting for diffuse coronary artery stenosis].Zhonghua Wai Ke Za Zhi. 2021 Feb 1;59(2):149-153. doi: 10.3760/cma.j.cn112139-20200203-00059. Zhonghua Wai Ke Za Zhi. 2021. PMID: 33378808 Chinese.
-
The midterm results of coronary endarterectomy in patients with diffuse coronary artery disease.J Cardiothorac Surg. 2018 Jul 24;13(1):90. doi: 10.1186/s13019-018-0776-8. J Cardiothorac Surg. 2018. PMID: 30041678 Free PMC article.
-
Left anterior descending coronary artery: long-term angiographic results of CABG with endarterectomy.J Cardiovasc Surg (Torino). 2007 Oct;48(5):633-40. J Cardiovasc Surg (Torino). 2007. PMID: 17989633
-
Does coronary endarterectomy technique affect surgical outcome when combined with coronary artery bypass grafting?Interact Cardiovasc Thorac Surg. 2014 Nov;19(5):848-55. doi: 10.1093/icvts/ivu261. Epub 2014 Aug 11. Interact Cardiovasc Thorac Surg. 2014. PMID: 25114125 Review.
-
Reusing the patent internal mammary artery as a conduit in redo coronary artery bypass surgery.Interact Cardiovasc Thorac Surg. 2016 Mar;22(3):346-50. doi: 10.1093/icvts/ivv338. Epub 2015 Dec 15. Interact Cardiovasc Thorac Surg. 2016. PMID: 26669852 Free PMC article. Review.
Cited by
-
Myocardial Perfusion Scan Study before and after On-Pump Coronary Artery Bypass Grafting Surgery - A Single-Center Study.Indian J Nucl Med. 2023 Jul-Sep;38(3):239-244. doi: 10.4103/ijnm.ijnm_162_22. Epub 2023 Oct 10. Indian J Nucl Med. 2023. PMID: 38046969 Free PMC article.
-
Comparing short and long term survival of patients undergoing off pump coronary artery bypass graft with and without coronary endarterectomy.Indian Heart J. 2017 Sep-Oct;69(5):646-650. doi: 10.1016/j.ihj.2017.02.008. Epub 2017 Feb 20. Indian Heart J. 2017. PMID: 29054191 Free PMC article.
-
Surgical coronary revascularization in patients with COVID-19; complications and outcomes: A retrospective cohort study.Health Sci Rep. 2022 Aug 10;5(5):e751. doi: 10.1002/hsr2.751. eCollection 2022 Sep. Health Sci Rep. 2022. PMID: 35957968 Free PMC article.
-
Predictors of Premature Mortality Following Coronary Artery Bypass Grafting: An Iranian Single-Centre Study.Healthcare (Basel). 2023 Dec 23;12(1):36. doi: 10.3390/healthcare12010036. Healthcare (Basel). 2023. PMID: 38200942 Free PMC article.
-
Anti-coagulation therapy following coronary endarterectomy in patient with coronary artery bypass graft.Caspian J Intern Med. 2018 Winter;9(1):27-31. doi: 10.22088/cjim.9.1.27. Caspian J Intern Med. 2018. PMID: 29387316 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Other Literature Sources