

Abdominal wall desmoid tumors: A proposal for US-guided resection
- PMID: 25706804
- PMCID: PMC4392329
- DOI: 10.1016/j.ijscr.2015.02.016
Abdominal wall desmoid tumors: A proposal for US-guided resection
Abstract
Background: Desmoid tumors (DTs) is a benign tumor with high tendency to infiltrative evolution and recurrence. Nowadays, in abdominal localization, the standard approach is surgery with R0 condition. The need to repair post-surgical wide wall defect requires conservative technique to decrease the incidence of incisional hernia and to obtain better quality of life (QoL).
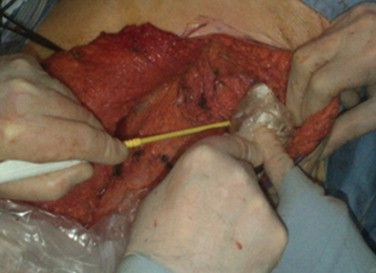
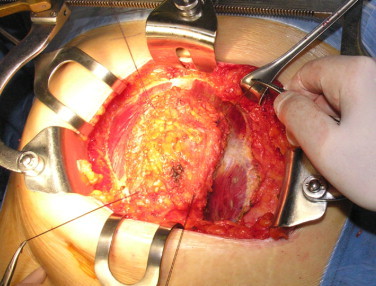
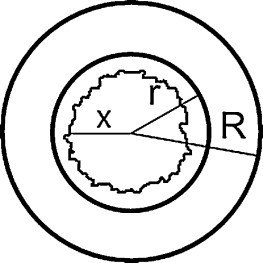
Methods: We perform an abdominal wall desmoid resection using ultrasound guide. This technique ensures to spare a wide wall area and to obtain a multilayer reconstruction minimizing postoperative risk. This approach allows good oncological results and better managing abdominal wall post-resection defect.
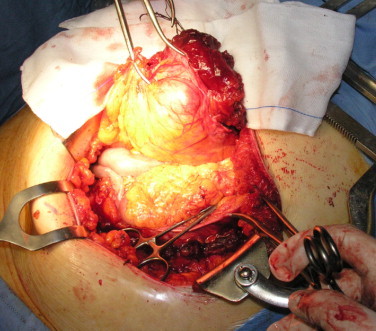
Results: We use US guided surgery to get radical approach and wall tissue spare that allows us a multilayer reconstruction minimizing post-operative complications. No recurrences were observed in one year follow up period.
Conclusion: Our experience represents first step to consider ultrasound mediated technique usefull to optimize wall resection surgery and to minimize following complications.
Keywords: Abdominal wall; Desmoid tumor; Oncological safety; Tissue sparing; Ultrasound.
Copyright © 2015 The Authors. Published by Elsevier Ltd.. All rights reserved.
Figures


References
-
- Fletcher C.D. Myofibroblastictumours: an update. VerhDtschGesPathol. 1998;82:75–82. - PubMed
-
- Kiel K.D., Suit H.D. Radiation therapy in the treatment of aggressive fibromatoses (desmoid tumors) Cancer. 1984;54:2051–2055. - PubMed
-
- Merchant N.B., Lewis J.J., Woodruff J.M., Leung D.H., Brennan M.F. Extremity and trunk desmoid tumors: a multifactorial analysis of outcome. Cancer. 1999;86:2045–2052. - PubMed
-
- Casillas J., Sais G.J., Greve J.L., Iparraguirre M.C., Morillo G. Imaging of intra- and extraabdominaldesmoid tumors. Radiographics. 1991;11:959–968. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
