

Neurogenic hyperadrenergic orthostatic hypotension: a newly recognized variant of orthostatic hypotension in older adults with elevated norepinephrine (noradrenaline)
- PMID: 25706983
- PMCID: PMC4417057
- DOI: 10.1042/CS20140766
Neurogenic hyperadrenergic orthostatic hypotension: a newly recognized variant of orthostatic hypotension in older adults with elevated norepinephrine (noradrenaline)
Abstract
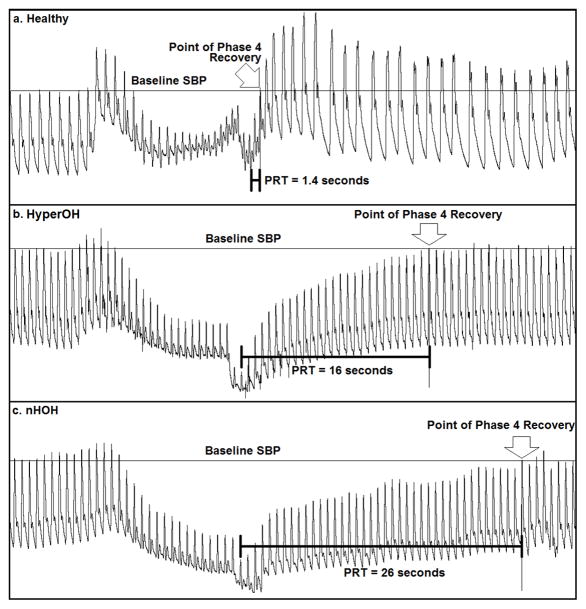
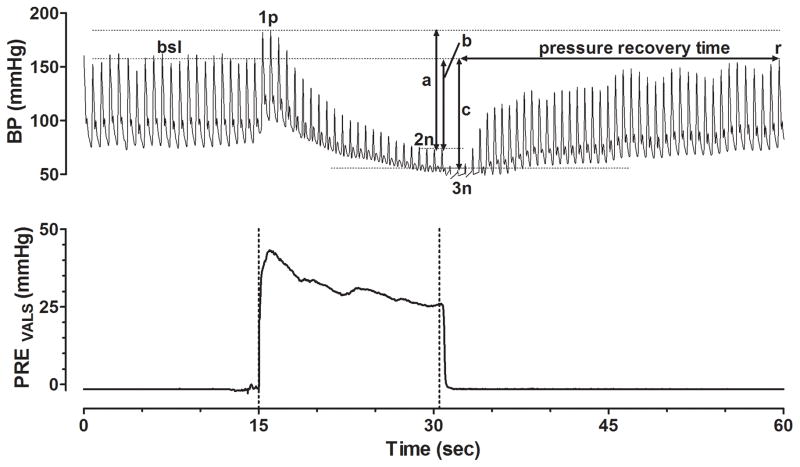
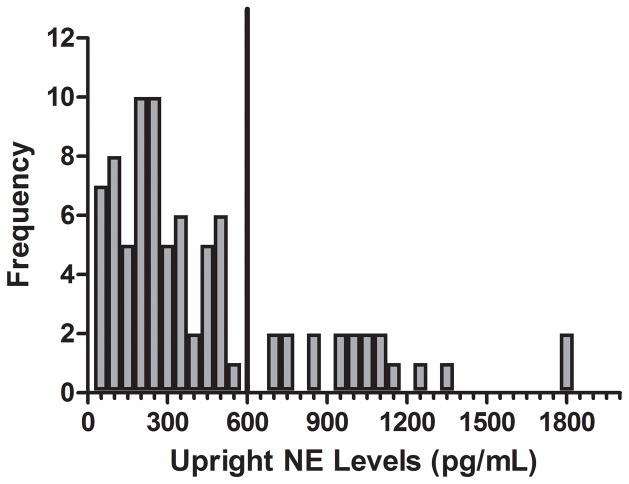
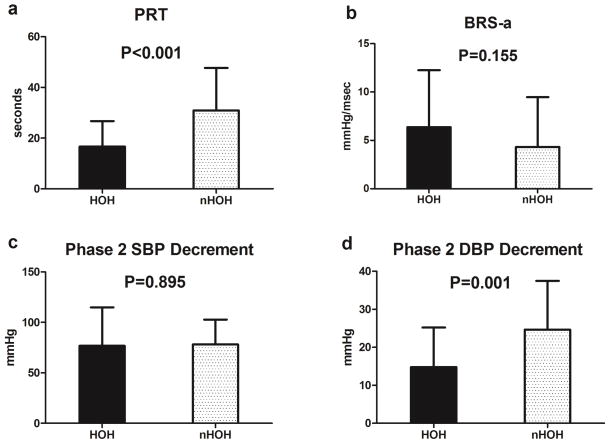
Patients with neurogenic orthostatic hypotension (OH) typically have impaired sympathetic nervous system tone and therefore low levels of upright plasma norepinephrine (NE) (noradrenaline). We report a subset of patients who clinically have typical neurogenic OH but who paradoxically have elevated upright levels of plasma NE. We retrospectively studied 83 OH patients evaluated at the Vanderbilt Autonomic Dysfunction Center between August 2007 and May 2013. Based on standing NE, patients were dichotomized into a hyperadrenergic OH group [hyperOH: upright NE ≥ 3.55 nmol/l (600 pg/ml), n=19] or a non-hyperadrenergic OH group [nOH: upright NE < 3.55 nmol/l (600 pg/ml), n=64]. Medical history and data from autonomic testing, including the Valsalva manoeuvre (VM), were analysed. HyperOH patients had profound orthostatic falls in blood pressure (BP), but less severe than in nOH [change in SBP (systolic blood pressure): -53 ± 31 mmHg compared with -68 ± 33 mmHg, P=0.050; change in DBP (diastolic blood pressure): -18 ± 23 mmHg compared with -30 ± 17 mmHg, P=0.01]. The expected compensatory increase in standing heart rate (HR) was similarly blunted in both hyperOH and nOH groups [84 ± 15 beats per minute (bpm) compared with 82 ± 14 bpm; P=0.6]. HyperOH patients had less severe sympathetic failure as evidenced by smaller falls in DBP during phase 2 of VM and a shorter VM phase 4 BP recovery time (16.5 ± 8.9 s compared with 31.6 ± 16.6 s; P<0.001) than nOH patients. Neurogenic hyperOH patients have severe neurogenic OH, but have less severe adrenergic dysfunction than nOH patients. Further work is required to understand whether hyperOH patients will progress to nOH or whether this represents a different disorder.
Figures
Similar articles
-
Characteristics of orthostatic hypotension in Parkinson's disease.Brain. 2007 Sep;130(Pt 9):2425-32. doi: 10.1093/brain/awm174. Epub 2007 Aug 2. Brain. 2007. Retraction in: Brain. 2008 Jun;131(Pt 6):1674. doi: 10.1093/brain/awn115. PMID: 17673498 Retracted.
-
Impaired cortical autonomic responses during sympathetic activation in neurogenic orthostatic hypotension characterized by postganglionic autonomic dysfunction.J Appl Physiol (1985). 2018 Oct 1;125(4):1210-1217. doi: 10.1152/japplphysiol.00245.2018. Epub 2018 Jun 14. J Appl Physiol (1985). 2018. PMID: 30332348
-
Validation of the new index of baroreflex function to identify neurogenic orthostatic hypotension.Auton Neurosci. 2020 Dec;229:102744. doi: 10.1016/j.autneu.2020.102744. Epub 2020 Nov 7. Auton Neurosci. 2020. PMID: 33189018
-
Diagnosing and treating neurogenic orthostatic hypotension in primary care.Postgrad Med. 2015;127(7):702-15. doi: 10.1080/00325481.2015.1050340. Epub 2015 May 27. Postgrad Med. 2015. PMID: 26012731 Review.
-
Neurogenic orthostatic hypotension in Parkinson's disease: evaluation, management, and emerging role of droxidopa.Vasc Health Risk Manag. 2014 Apr 3;10:169-76. doi: 10.2147/VHRM.S53983. eCollection 2014. Vasc Health Risk Manag. 2014. PMID: 24729712 Free PMC article. Review.
Cited by
-
Standardized Autonomic Testing in Patients With Probable Radiation-Induced Afferent Baroreflex Failure.Hypertension. 2022 Jan;79(1):50-56. doi: 10.1161/HYPERTENSIONAHA.121.17805. Epub 2021 Nov 5. Hypertension. 2022. PMID: 34739766 Free PMC article.
-
Neurogenic orthostatic hypotension after treatment with sorafenib.BMJ Case Rep. 2022 Dec 22;15(12):e247140. doi: 10.1136/bcr-2021-247140. BMJ Case Rep. 2022. PMID: 36549761 Free PMC article.
-
Different phenoconversion pathways in pure autonomic failure with versus without Lewy bodies.Clin Auton Res. 2021 Dec;31(6):677-684. doi: 10.1007/s10286-021-00829-y. Epub 2021 Oct 20. Clin Auton Res. 2021. PMID: 34669076 Free PMC article. Review.
-
Hyperadrenergic Orthostatic Hypotension With Pure Peripheral Sympathetic Denervation Associated With Sjogren's Syndrome.Cureus. 2021 Sep 7;13(9):e17805. doi: 10.7759/cureus.17805. eCollection 2021 Sep. Cureus. 2021. PMID: 34660015 Free PMC article.
-
Hyperadrenergic Postural Tachycardia Syndrome: Clinical Biomarkers and Response to Guanfacine.Hypertension. 2024 Nov;81(11):2237-2247. doi: 10.1161/HYPERTENSIONAHA.124.23035. Epub 2024 Aug 7. Hypertension. 2024. PMID: 39109428
References
-
- Freeman R, Wieling W, Axelrod FB, et al. Consensus statement on the definition of orthostatic hypotension, neurally mediated syncope and the postural tachycardia syndrome. Clin Auton Res. 2011;21:69–72. - PubMed
-
- Low PA. Prevalence of orthostatic hypotension. Clin Auton Res. 2008;18(Suppl 1):8–13. - PubMed
-
- Poon IO, Braun U. High prevalence of orthostatic hypotension and its correlation with potentially causative medications among elderly veterans. J Clin Pharm Ther. 2005;30:173–178. - PubMed
-
- Shibao C, Grijalva CG, Raj SR, Biaggioni I, Griffin MR. Orthostatic hypotension-related hospitalizations in the United States. Am J Med. 2007;120:975–980. - PubMed
-
- Robertson D, Robertson RM. Causes of chronic orthostatic hypotension. Arch Intern Med. 1994;154:1620–1624. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources