

The pathogenesis of pediatric cerebral malaria: eye exams, autopsies, and neuroimaging
- PMID: 25708306
- PMCID: PMC4405463
- DOI: 10.1111/nyas.12690
The pathogenesis of pediatric cerebral malaria: eye exams, autopsies, and neuroimaging
Abstract
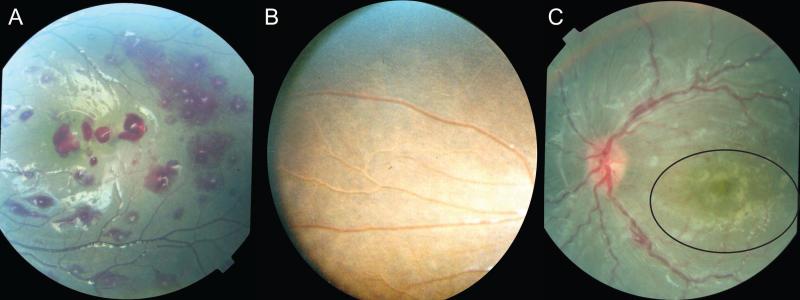
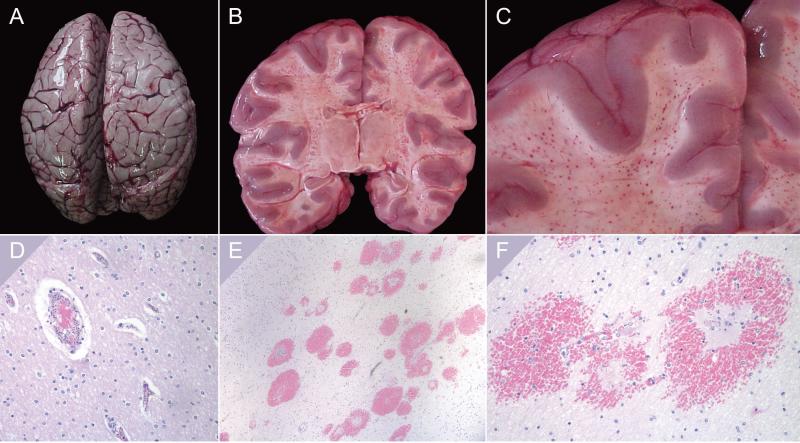
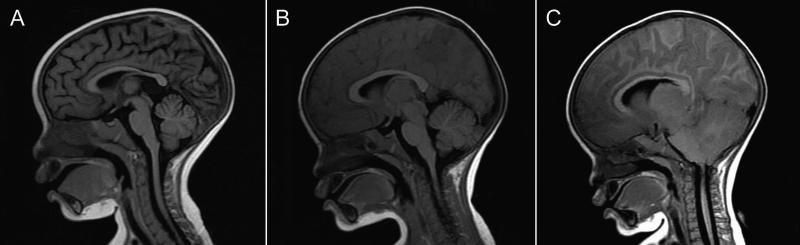
Several advances in our understanding of pediatric cerebral malaria (CM) have been made over the past 25 years. Accurate clinical diagnosis is enhanced by the identification of a characteristic retinopathy, visible by direct or indirect ophthalmoscopy, the retinal changes (retinal whitening, vessel color changes, white-centered hemorrhages) being consistently associated with intracerebral sequestration of parasites in autopsy studies. Autopsies have yielded information at tissue levels in fatal CM, but new insights into critical pathogenetic processes have emerged from neuroimaging studies, which, unlike autopsy-based studies, permit serial observations over time and allow comparisons between fatal cases and survivors. Brain swelling has emerged as the major risk factor for death, and, among survivors, brain volume diminishes spontaneously over 24-48 hours. Studies of life-threatening and fatal malaria are suggesting new approaches to identifying and caring for those at highest risk; potential adjuvants should be evaluated and implemented where they are most needed.
Keywords: African children; brain swelling; cerebral malaria; pathogenesis; sequestration.
© 2015 New York Academy of Sciences.
Figures
References
-
- Dondorp A, Nosten F, Stepniewska K, et al. Artesunate versus quinine for treatment of severe falciparum malaria: a randomised trial. Lancet. 2005;366:717–725. - PubMed
-
- Warrell DA, Looareesuwan S, Warrell MJ, et al. Dexamethasone proves deleterious in cerebral malaria. A double-blind trial in 100 comatose patients. N Engl J Med. 1982;306:313–319. - PubMed
-
- Molyneux ME, Taylor TE, Wirima JJ, et al. Clinical features and prognostic indicators in paediatric cerebral malaria: a study of 131 comatose Malawian children. Q J Med. 1989;71:441–459. - PubMed
-
- Newton CR, Chokwe T, Schellenberg JA, et al. Coma scales for children with severe falciparum malaria. Trans R Soc Trop Med Hyg. 1997;91:161–165. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
