

Hyoid myotomy without suspension: a surgical approach to obstructive sleep apnoea syndrome
- PMID: 25709152
- PMCID: PMC4299162
Hyoid myotomy without suspension: a surgical approach to obstructive sleep apnoea syndrome
Abstract
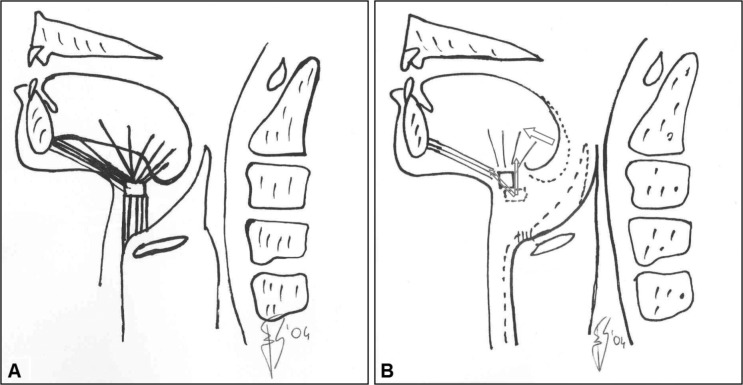
The aim of this study was to verify if hyoid myotomy without hyoid suspension is effective in surgical treatment of obstructive sleep apnoea syndrome (OSAS). We recruited six patients with OSAS, aged between 34 to 60 years, with retropalatal and retrolingual upper airway obstruction, non-obese (BMI < 27) and non-compliant to continuous positive airway pressure therapy. Pre-surgical clinical and instrumental evaluations included clinical examination, cephalometry, polysomnography (PSG) and sleep endoscopy. Surgical treatment included nasal surgery, uvulopalatopharyngoplasty, tonsillectomy and hyoid myotomy without hyoid suspension. Follow-up evaluations were performed with serial PSGs, performed early (one week after surgery), and at 1, 6 and 18 months after surgery. We observed that surgery was followed by immediate normalisation of breathing parameters evaluated by PSG that persisted after 18 months. Thus, hyoid myotomy without suspension combined with nasal and palatal surgery may be considered a valid treatment of non-obese OSAS patients with retrolingual and retropalatal collapse. Furthermore, we suggest that hyoid bone suspension, binding it to mandibular or to thyroid cartilage, might be unnecessary in selected cases.
Obiettivo di questo studio è stato verificare se la miotomia ioidea senza sospensione è efficace nel trattamento chirurgico della sindrome delle apnee ostruttive del sonno (OSAS) nell'ambito del primo step della chirurgia multilivello. Abbiamo reclutato sei pazienti affetti da OSAS, di età compresa tra i 34 e i 60 anni, con un'ostruzione delle alte vie aeree a livello retropalatale e retrolinguale, non obesi (BMI <27) e che mostravano scarsa tolleranza nei confronti della terapia con ventilazione meccanica a pressione positiva continua delle alte vie aeree. Durante la valutazione clinica pre-intervento i pazienti sono stati sottoposti a esame clinico otorinolaringoiatrico, cefalometria, polisonnografia (PSG) e sleep-endoscopy. Tutti i pazienti sono stati sottoposti nella stessa seduta a chirurgia nasale, uvulopalatofaringoplastica, tonsillectomia e miotomia ioidea senza sospensione. Nel corso del follow-up i pazienti sono stati sottoposti a PSG seriali, all'inizio (una settimana dopo l'intervento chirurgico), ed a 1, 6 e 18 mesi dopo l'intervento chirurgico. I dati polisonnografici hanno messo in evidenza un significativo miglioramento dei parametri respiratori nell'immediato post operatorio che si è mantenuto stabile per almeno 18 mesi. Alla luce della nostra analisi preliminare l'intervento di miotomia ioidea senza sospensione in combinazione con la chirurgia nasale e palatale può essere considerato un valido trattamento per i pazienti affetti da OSAS, non obesi, con collasso delle alte vie aeree a livello retrolinguale e retropalatale. Per tale motivo la sospensione ioidea, con ancoraggio alla mandibola o alla cartilagine tiroidea, in alcuni casi selezionati, potrebbe non essere necessaria.
Keywords: Hyoid myotomy; Obstructive sleep apnoea syndrome; Sub-hyoid muscles; Uvulopalatopharyngoplasty.
Figures
References
-
- Fujita S. Midline laser glossectomy with linguoplasty: a treatment of sleep apnea syndrome. Op Tech Otolaryngol HNS. 1991;2:127–131.
-
- Sher AE, Schechtman KB, Piccirillo F. The efficacy of surgical modifications of the upper airway in adults with obstructive sleep apnea syndrome. An American sleep disorders association review. Sleep. 1996;19:156–177. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources