

MR defecography for obstructed defecation syndrome
- PMID: 25709162
- PMCID: PMC4329684
- DOI: 10.4103/0971-3026.150134
MR defecography for obstructed defecation syndrome
Abstract
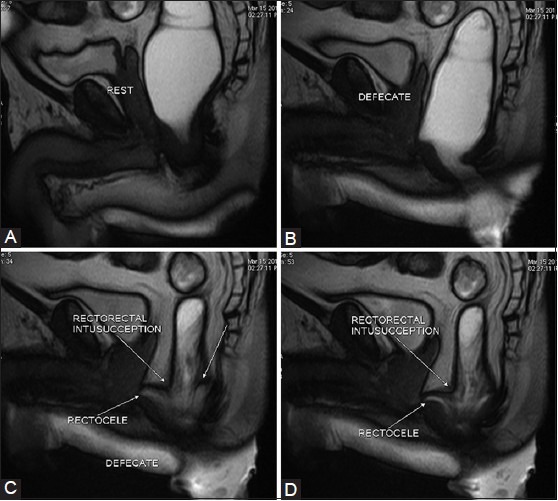
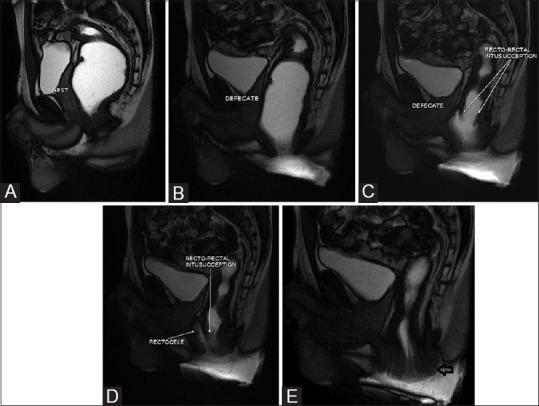
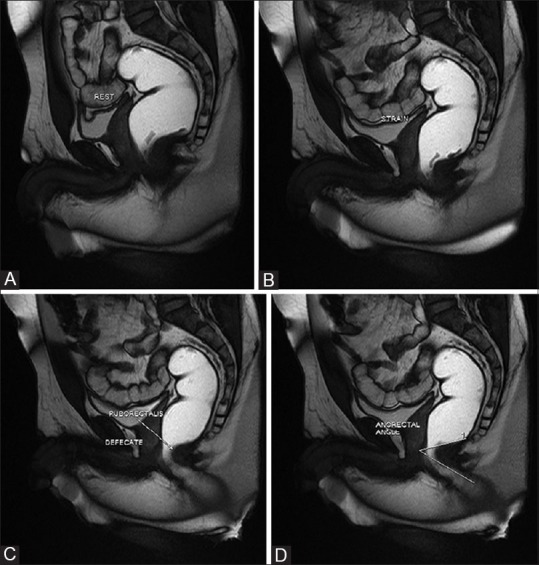
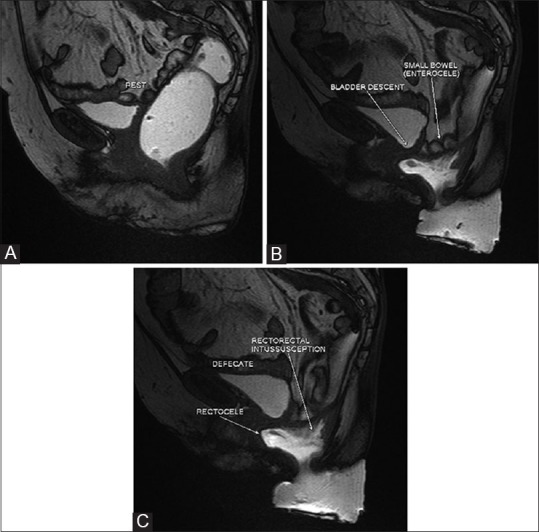
Patients with obstructed defecation syndrome (ODS) form an important subset of patients with chronic constipation. Evaluation and treatment of these patients has traditionally been difficult. Magnetic resonance defecography (MRD) is a very useful tool for the evaluation of these patients. We evaluated the scans and records of 192 consecutive patients who underwent MRD at our center between January 2011 and January 2012. Abnormal descent, rectoceles, rectorectal intussusceptions, enteroceles, and spastic perineum were observed in a large number of these patients, usually in various combinations. We discuss the technique, its advantages and limitations, and the normal findings and various pathologies.
Keywords: Chronic constipation; magnetic resonance defecography; obstructed defecation syndrome; pelvic floor.
Conflict of interest statement
Figures
Similar articles
-
The clinical value of magnetic resonance defecography in males with obstructed defecation syndrome.Tech Coloproctol. 2018 Mar;22(3):179-190. doi: 10.1007/s10151-018-1759-4. Epub 2018 Mar 6. Tech Coloproctol. 2018. PMID: 29512048
-
Dynamic transperineal ultrasound in the workup of men with obstructed defecation: a pilot study.Dis Colon Rectum. 2012 Sep;55(9):976-82. doi: 10.1097/DCR.0b013e31825ef8ec. Dis Colon Rectum. 2012. PMID: 22874605
-
Magnetic resonance defecography assessment of obstructed defecation syndrome in patients with chronic constipation in a tertiary care hospital.World J Radiol. 2025 May 28;17(5):106102. doi: 10.4329/wjr.v17.i5.106102. World J Radiol. 2025. PMID: 40503482 Free PMC article.
-
Role of magnetic resonance defecography in the assessment of obstructed defecation syndrome.World J Radiol. 2025 Jun 28;17(6):107205. doi: 10.4329/wjr.v17.i6.107205. World J Radiol. 2025. PMID: 40606048 Free PMC article. Review.
-
[Differential diagnosis in descending perineum syndrome].Chirurg. 2004 Sep;75(9):850-60. doi: 10.1007/s00104-004-0922-9. Chirurg. 2004. PMID: 15258747 Review. German.
Cited by
-
Imaging of pelvic floor disorders involving the posterior compartment on dynamic MR defaecography.SA J Radiol. 2024 Oct 11;28(1):2935. doi: 10.4102/sajr.v28i1.2935. eCollection 2024. SA J Radiol. 2024. PMID: 39506983 Free PMC article.
-
Evaluation, Diagnosis, and Medical Management of Rectal Prolapse.Clin Colon Rectal Surg. 2017 Feb;30(1):16-21. doi: 10.1055/s-0036-1593431. Clin Colon Rectal Surg. 2017. PMID: 28144208 Free PMC article. Review.
-
Chronic constipation in Rome IV era: The Indian perspective.Indian J Gastroenterol. 2017 May;36(3):163-173. doi: 10.1007/s12664-017-0757-1. Epub 2017 Jun 23. Indian J Gastroenterol. 2017. PMID: 28643273 Review.
-
Diagnostic approach to faecal incontinence: What test and when to perform?World J Gastroenterol. 2021 Apr 21;27(15):1553-1562. doi: 10.3748/wjg.v27.i15.1553. World J Gastroenterol. 2021. PMID: 33958842 Free PMC article. Review.
-
Chronic constipation: A review of literature.Medicine (Baltimore). 2018 May;97(20):e10631. doi: 10.1097/MD.0000000000010631. Medicine (Baltimore). 2018. PMID: 29768326 Free PMC article.
References
-
- Longstreth GF, Thompson WG, Chey WD, Houghton LA, Mearin F, Spiller RC. Functional bowel disorders. Gastroenterology. 2006;130:1480–91. - PubMed
-
- Sonnenberg A, Koch TR. Physician visits in the United States for constipation: 1958 to 1986. Dig Dis Sci. 1989;34:606–11. - PubMed
-
- Lembo A, Camilleri M. Chronic constipation. N Engl J Med. 2003;349:1360–8. - PubMed
-
- National Institute for Health and Clinical Excellence. Stapled Transanal Rectal Resection for Obstructed Defecation Syndrome. NICE Interventional Procedure Guidance (IPG 351) Issued June 2010. [Last accessed on 2014 Jun 20]. Available from: http://www.nice.org.uk .
-
- Kelvin FM, Maglinte DD, Hale DS, Benson JT. Female pelvic organ prolapse: A comparison of triphasic dynamic MR imaging and triphasic fluoroscopic cystocolpoproctography. AJR Am J Roentgenol. 2000;174:81–8. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources