

Initial Treatment of Respiratory Distress Syndrome with Nasal Intermittent Mandatory Ventilation versus Nasal Continuous Positive Airway Pressure: A Randomized Controlled Trial
- PMID: 25709790
- PMCID: PMC4336985
Initial Treatment of Respiratory Distress Syndrome with Nasal Intermittent Mandatory Ventilation versus Nasal Continuous Positive Airway Pressure: A Randomized Controlled Trial
Abstract
Background: Neonatal respiratory distress syndrome (RDS) in premature infants who survived and its complications are a common problem. Due to high morbidity and mechanical ventilation (MV) nowadays researchers in interested minimizing MV. To determine, in very low birth weight (BW) preterm neonates with RDS, if initial treatment with nasal intermittent mandatory ventilation (early NIMV) compared with early nasal continuous positive airway pressure (early NCPAP) obtains more favorable outcomes in terms of the duration of treatment, and the need for endotracheal tube ventilation.
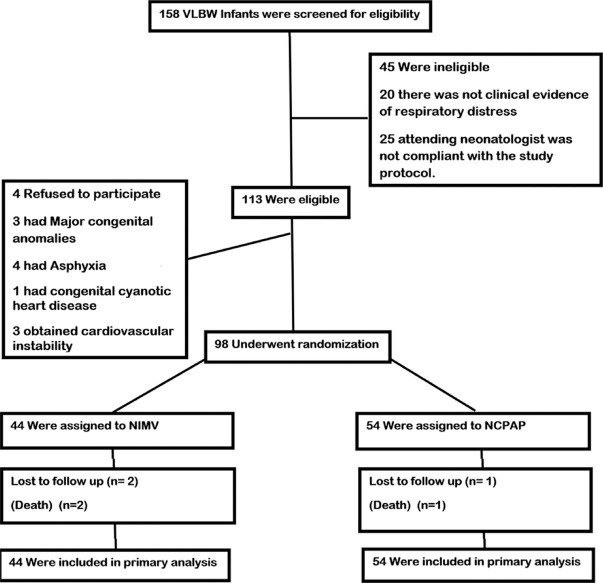
Methods: In this single-center randomized control trial study, infants (BW ≤ 1500 g and/or gestational age ≤ 34 weeks) with respiratory distress were considered eligible. Forty-four infants were randomly assigned to receive early-NIMV and 54 comparable infants to early-NCPAP. Surfactants were given, when FIO2 requirement was of >30%. Primary outcomes were failure of noninvasive respiratory support, that is, the need for MV in the first 48 h of life and for the duration of noninvasive respiratory support in each group.
Results: 98 infants were enrolled (44 in the NIMV and 54 in the NCPAP group). The Preventive power of MV of NIMV usage (95.5%) was not lower than the NCPAP (98.1%) strength (hazard ratio: 0.21 (95% confidence interval: 0.02-2.66); P: 0.23). The duration of noninvasive respiratory support in the NIMV group was significantly shorter than NCPAP (the median (range) was 24 (18.00-48.00) h versus 48.00 (22.00-120.00) h in NIMV versus NCPAP groups; P < 0.001). Similarly, the duration of dependency on oxygen was less, for NIMV (the median (range) was 96.00 (41.00-504.00) h versus144.00 (70.00-1130.00) h in NIMV versus NCPAP groups; P: 0.009). Interestingly, time to full enteral feeds and length of hospital stay were more favorable in the NIMV versus the NCPAP group.
Conclusions: Initial treatment of RDS with NIMV was safe, and well tolerated. Furthermore, NIMV had excellent benefits such as reduction of the duration of treatment, oxygen dependency period and length of hospital stay. Therefore, the primary mode with NIMV could be a feasible method of noninvasive ventilation in very premature infants.
Keywords: Nasal CPAP; noninvasive ventilation; premature infants; respiratory distress syndrome; surfactant.
Conflict of interest statement
References
-
- Seki K, Iwasaki S, An H, Horiguchi H, Mori M, Nishimaki S, et al. Early discharge from a neonatal intensive care unit and rates of readmission. Pediatr Int. 2011;53:7–12. - PubMed
-
- Mathews TJ, MacDorman MF. Infant mortality statistics from the 2008 period linked birth/infant death data set. Natl Vital Stat Rep. 2012;60:1–27. - PubMed
-
- Kugelman A, Feferkorn I, Riskin A, Chistyakov I, Kaufman B, Bader D. Nasal intermittent mandatory ventilation versus nasal continuous positive airway pressure for respiratory distress syndrome: A randomized, controlled, prospective study. J Pediatr. 2007;150:521–6. 5261. - PubMed
-
- Thomson MA IFDAS Study Group. Early nasal continuous positive pressure with prophylactic surfactant for neonates at risk of RDS. The IFDAS Multi-Center randomized trial. Pediatr Res. 2002;51:379A.
-
- Polin RA, Sahni R. Newer experience with CPAP. Semin Neonatol. 2002;7:379–89. - PubMed
LinkOut - more resources
Full Text Sources
Medical