

Spatial and temporal heterogeneity in high-grade serous ovarian cancer: a phylogenetic analysis
- PMID: 25710373
- PMCID: PMC4339382
- DOI: 10.1371/journal.pmed.1001789
Spatial and temporal heterogeneity in high-grade serous ovarian cancer: a phylogenetic analysis
Abstract
Background: The major clinical challenge in the treatment of high-grade serous ovarian cancer (HGSOC) is the development of progressive resistance to platinum-based chemotherapy. The objective of this study was to determine whether intra-tumour genetic heterogeneity resulting from clonal evolution and the emergence of subclonal tumour populations in HGSOC was associated with the development of resistant disease.
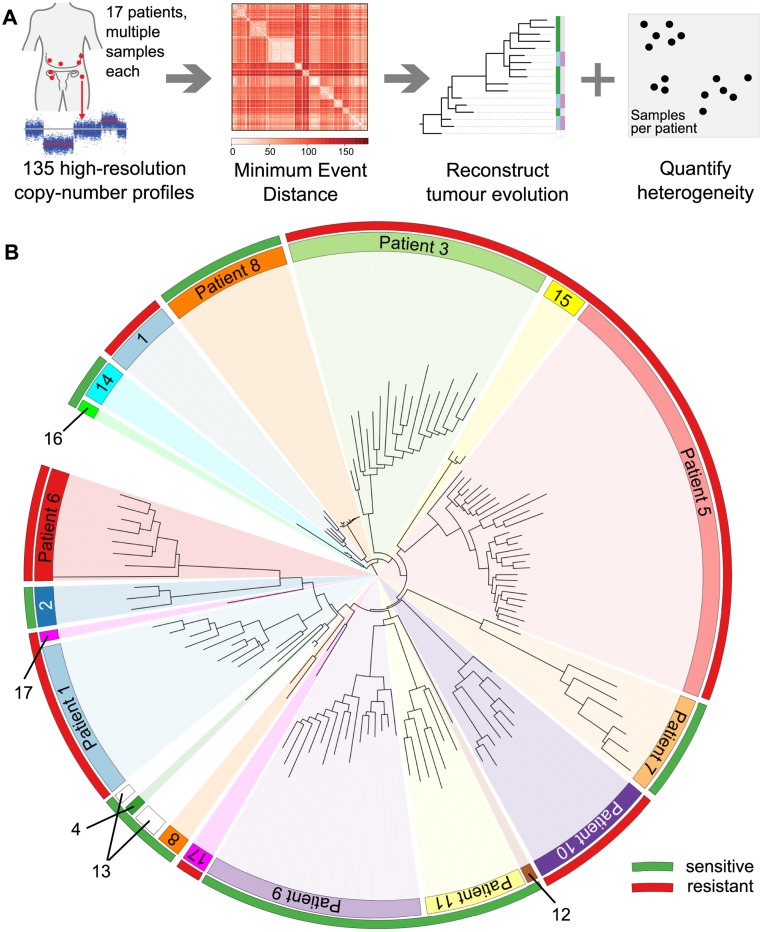
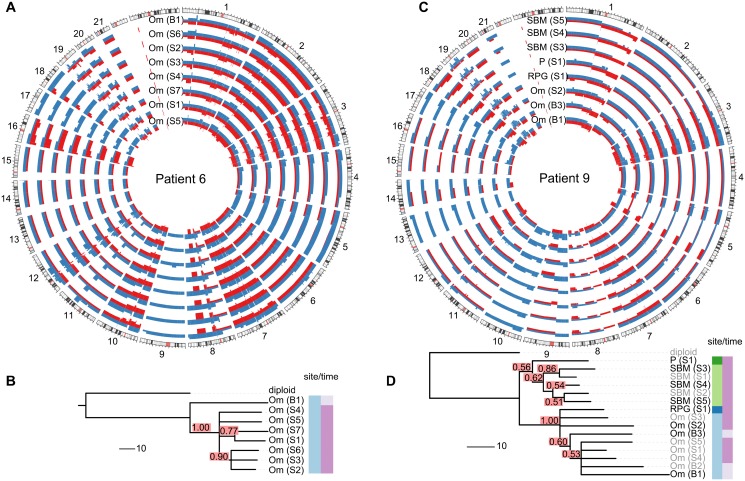
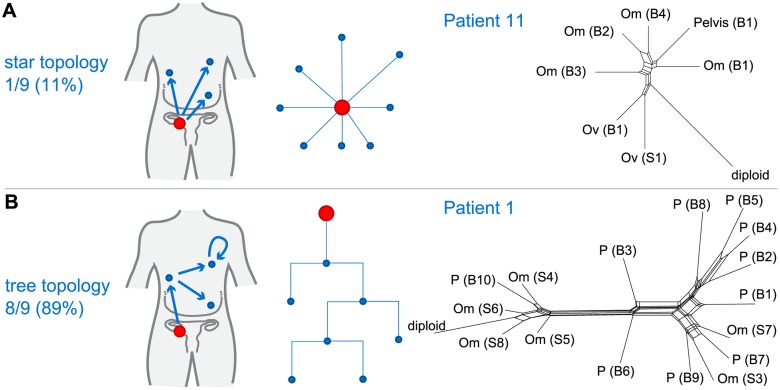
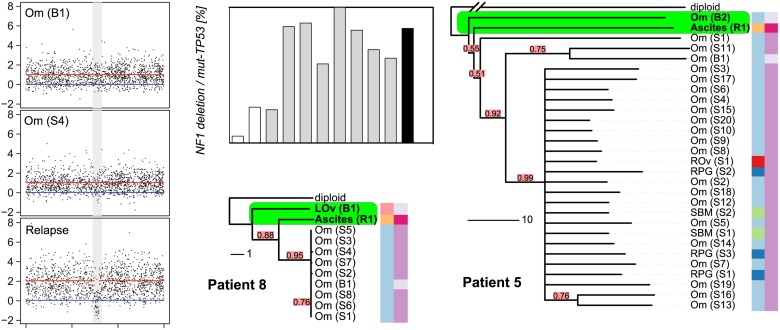
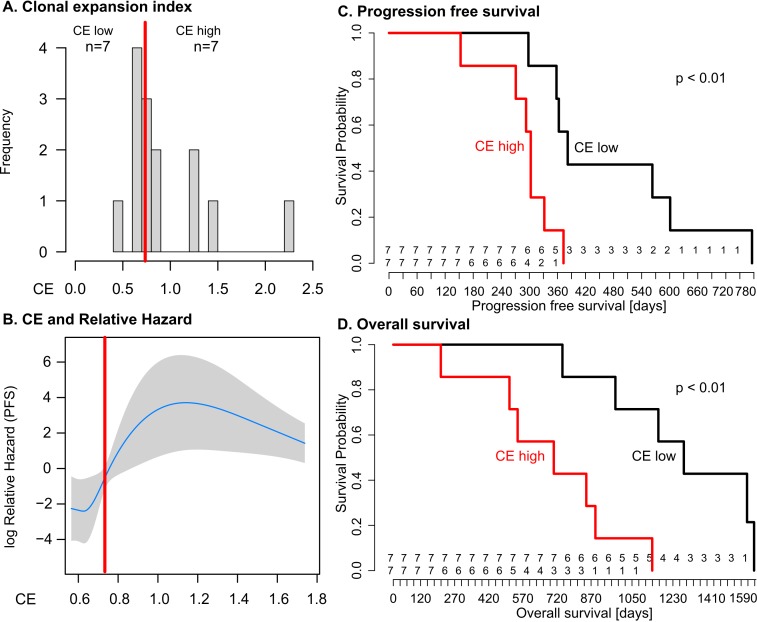
Methods and findings: Evolutionary inference and phylogenetic quantification of heterogeneity was performed using the MEDICC algorithm on high-resolution whole genome copy number profiles and selected genome-wide sequencing of 135 spatially and temporally separated samples from 14 patients with HGSOC who received platinum-based chemotherapy. Samples were obtained from the clinical CTCR-OV03/04 studies, and patients were enrolled between 20 July 2007 and 22 October 2009. Median follow-up of the cohort was 31 mo (interquartile range 22-46 mo), censored after 26 October 2013. Outcome measures were overall survival (OS) and progression-free survival (PFS). There were marked differences in the degree of clonal expansion (CE) between patients (median 0.74, interquartile range 0.66-1.15), and dichotimization by median CE showed worse survival in CE-high cases (PFS 12.7 versus 10.1 mo, p = 0.009; OS 42.6 versus 23.5 mo, p = 0.003). Bootstrap analysis with resampling showed that the 95% confidence intervals for the hazard ratios for PFS and OS in the CE-high group were greater than 1.0. These data support a relationship between heterogeneity and survival but do not precisely determine its effect size. Relapsed tissue was available for two patients in the CE-high group, and phylogenetic analysis showed that the prevalent clonal population at clinical recurrence arose from early divergence events. A subclonal population marked by a NF1 deletion showed a progressive increase in tumour allele fraction during chemotherapy.
Conclusions: This study demonstrates that quantitative measures of intra-tumour heterogeneity may have predictive value for survival after chemotherapy treatment in HGSOC. Subclonal tumour populations are present in pre-treatment biopsies in HGSOC and can undergo expansion during chemotherapy, causing clinical relapse.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Nowell PC (1976) The clonal evolution of tumor cell populations. Science 194: 23–28. - PubMed
-
- Dexter DL, Kowalski HM, Blazar BA, Fligiel Z, Vogel R, et al. (1978) Heterogeneity of tumor cells from a single mouse mammary tumor. Cancer Res 38: 3174–3181. - PubMed
-
- Khalique L, Ayhan A, Weale ME, Jacobs IJ, Ramus SJ, et al. (2007) Genetic intra-tumour heterogeneity in epithelial ovarian cancer and its implications for molecular diagnosis of tumours. J Pathol 211: 286–295. - PubMed
Publication types
MeSH terms
Substances
Associated data
- Actions
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
