

Traditional Chinese medicine for neck pain and low back pain: a systematic review and meta-analysis
- PMID: 25710765
- PMCID: PMC4339195
- DOI: 10.1371/journal.pone.0117146
Traditional Chinese medicine for neck pain and low back pain: a systematic review and meta-analysis
Abstract
Background: Neck pain (NP) and low back pain (LBP) are common symptoms bothering people in daily life. Traditional Chinese medicine (TCM) has been used to treat various symptoms and diseases in China and has been demonstrated to be effective. The objective of the present study was to review and analyze the existing data about pain and disability in TCM treatments for NP and LBP.
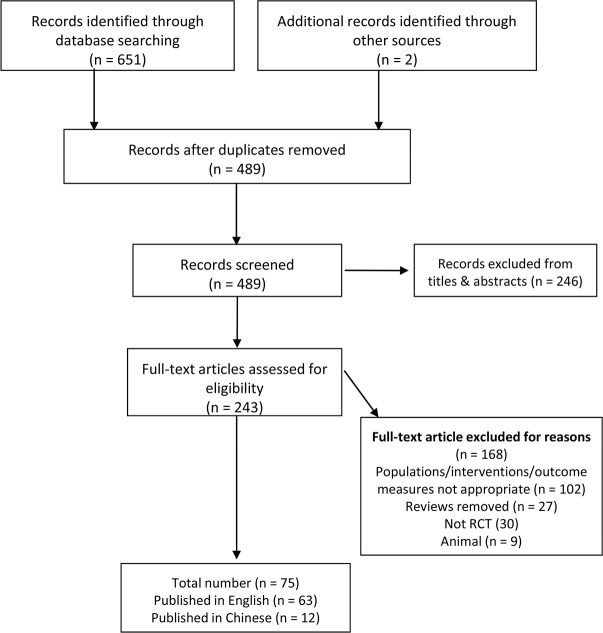
Methods: Studies were identified by a comprehensive search of databases, such as MEDLINE, EMBASE, and Cochrane Library, up to September 1, 2013. A meta-analysis was performed to evaluate the efficacy and safety of TCM in managing NP and LBP.
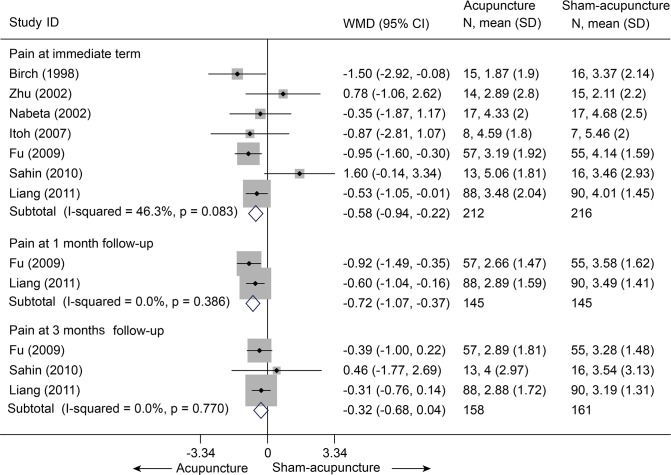
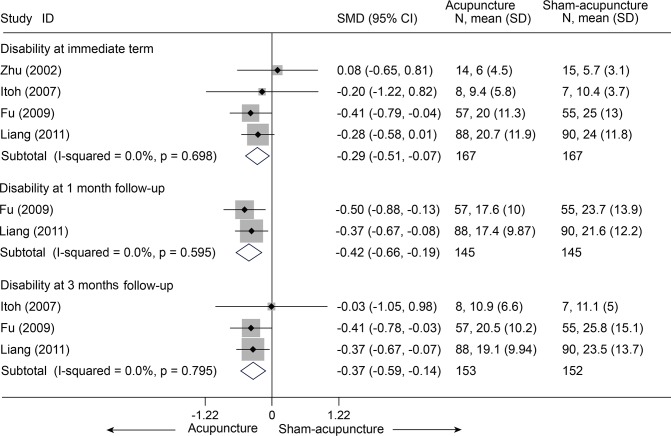
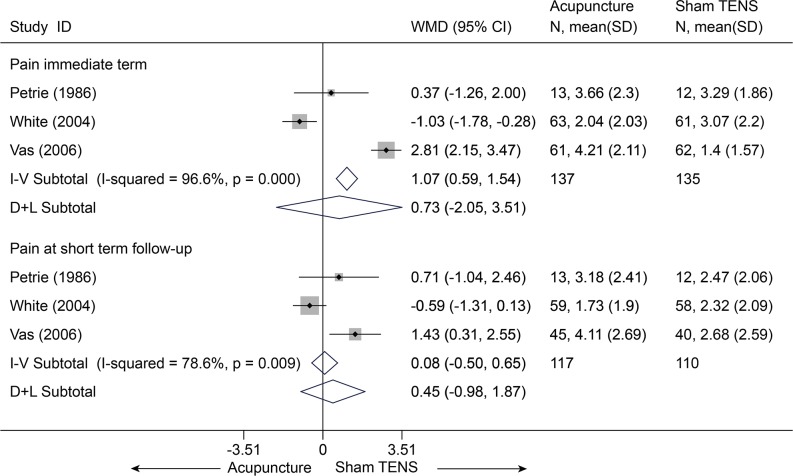
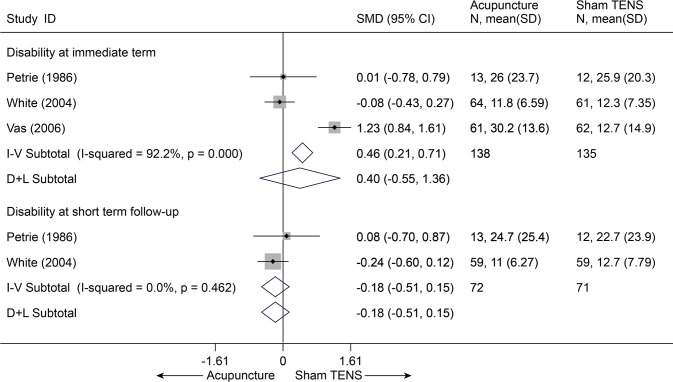
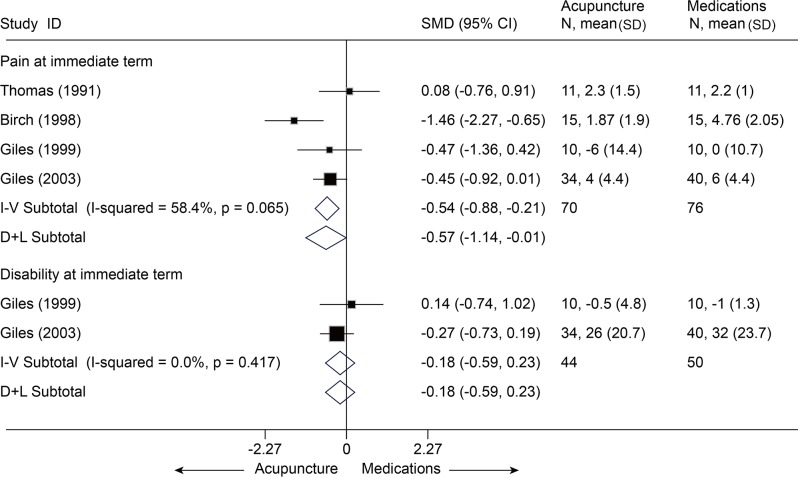
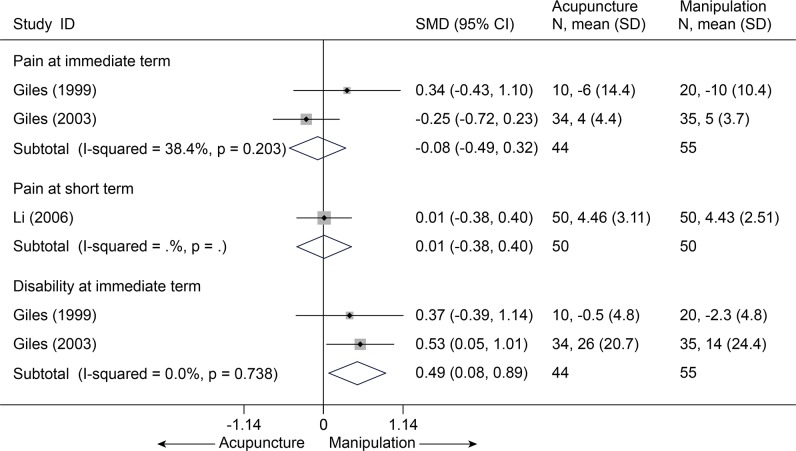
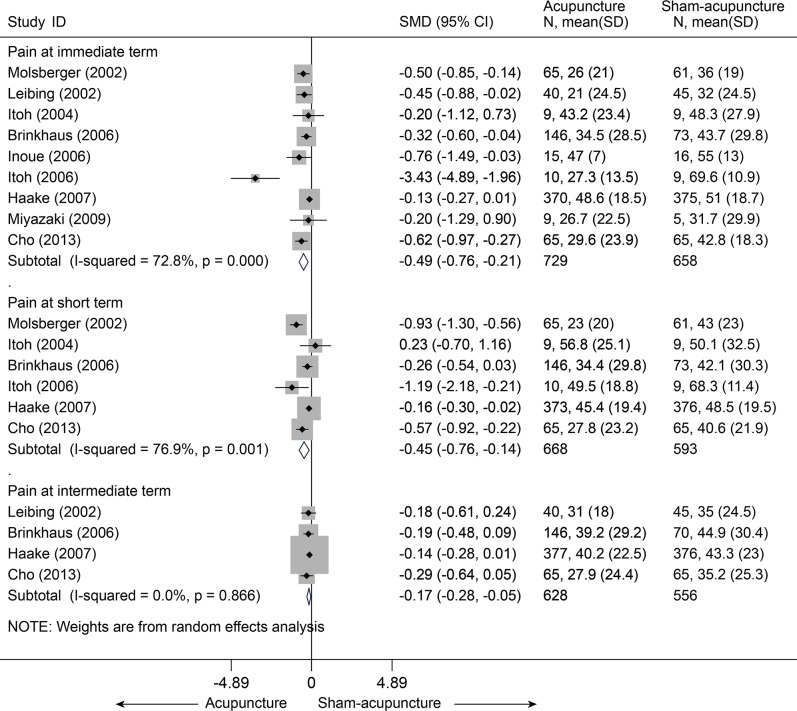
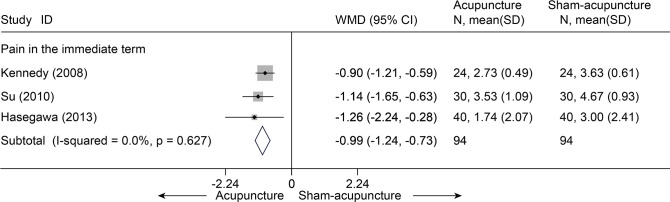
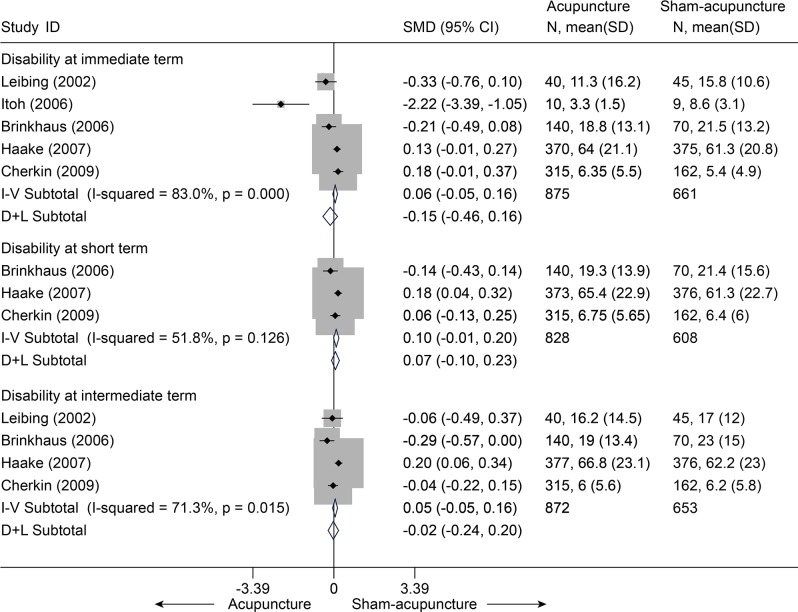
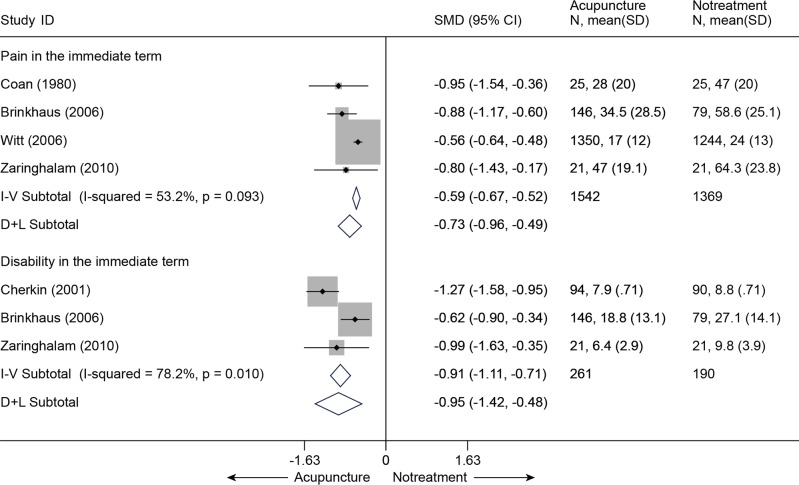
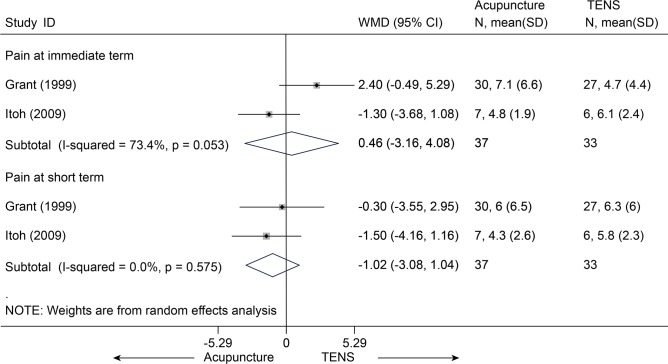
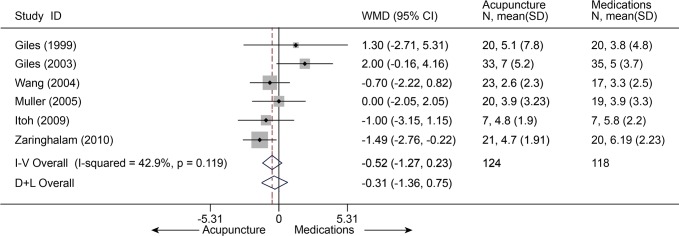
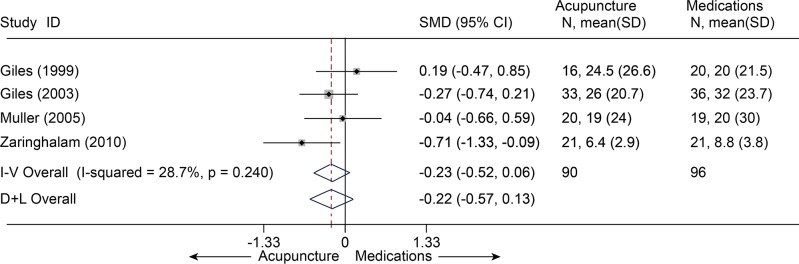
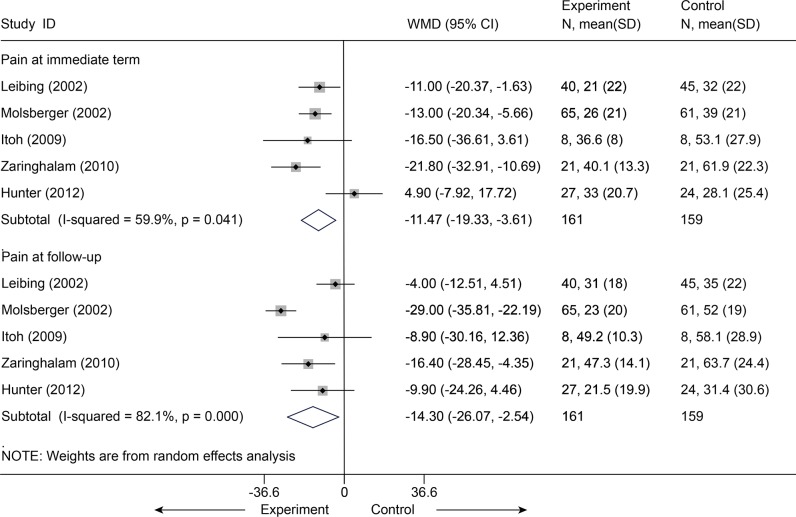
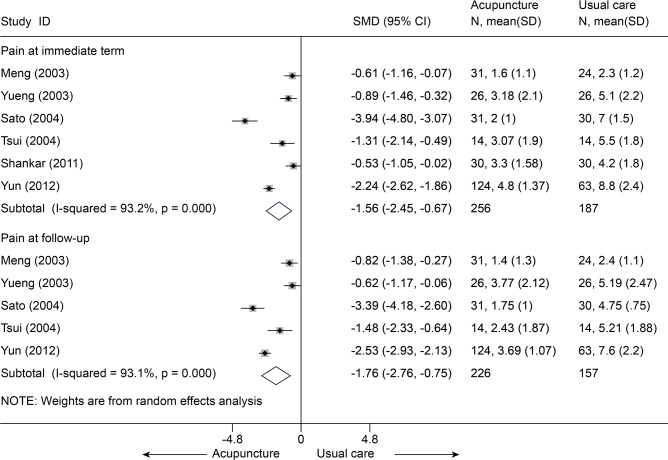
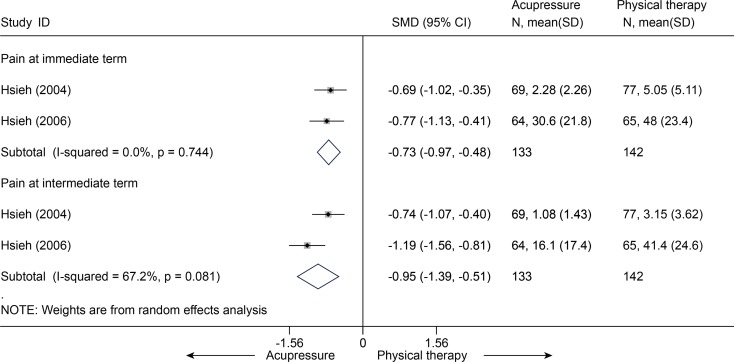
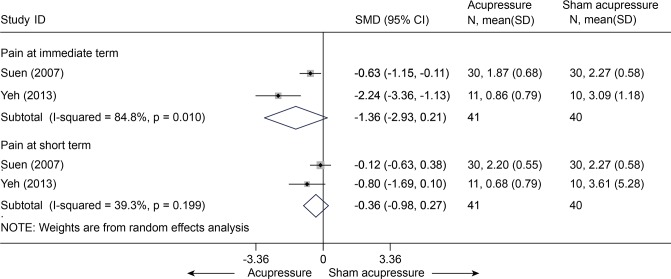
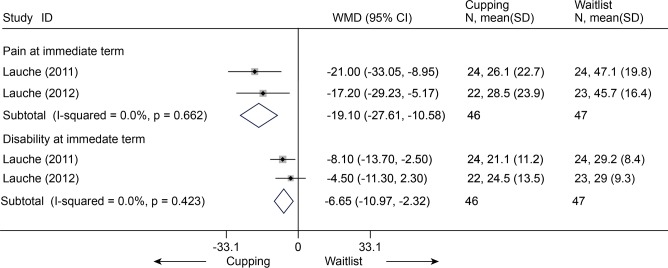
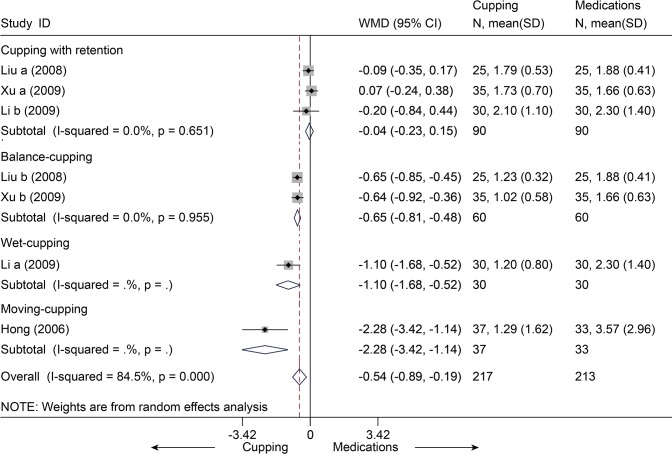
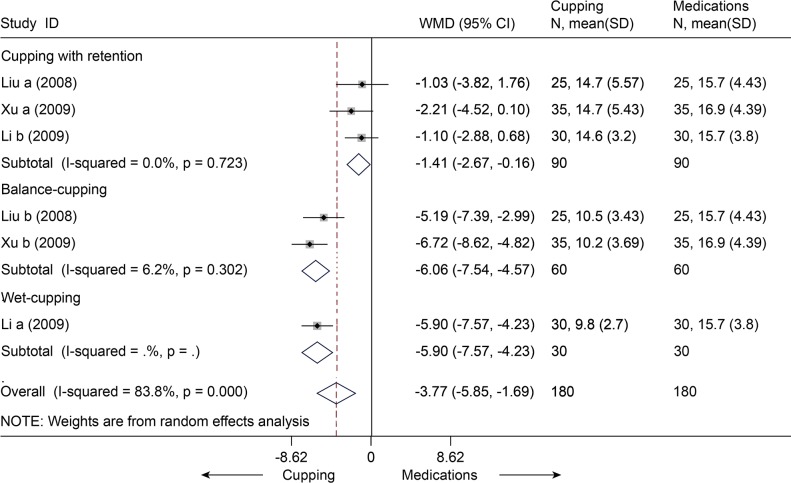
Results: Seventy five randomized controlled trials (n = 11077) were included. Almost all of the studies investigated individuals experiencing chronic NP (CNP) or chronic LBP (CLBP). We found moderate evidence that acupuncture was more effective than sham-acupuncture in reducing pain immediately post-treatment for CNP (visual analogue scale (VAS) 10 cm, mean difference (MD) = -0.58 (-0.94, -0.22), 95% confidence interval, p = 0.01), CLBP (standardized mean difference = -0.47 (-0.77, -0.17), p = 0.003), and acute LBP (VAS 10 cm, MD = -0.99 (-1.24, -0.73), p< 0.001). Cupping could be more effective than waitlist in VAS (100 mm) (MD = -19.10 (-27.61, -10.58), p < 0. 001) for CNP or medications (e.g. NSAID) for CLBP (MD = -5.4 (-8.9, -0.19), p = 0.003). No serious or life-threatening adverse effects were found.
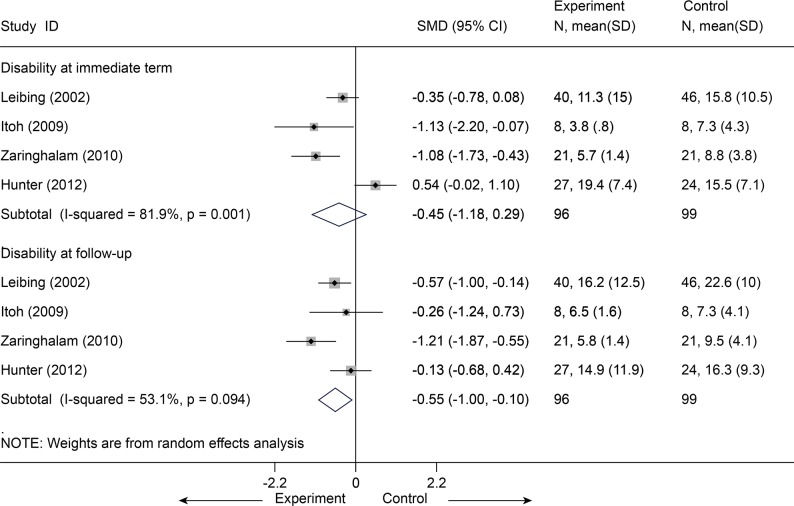
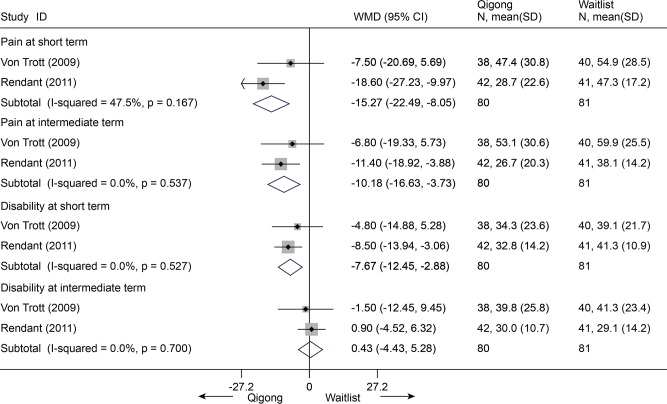
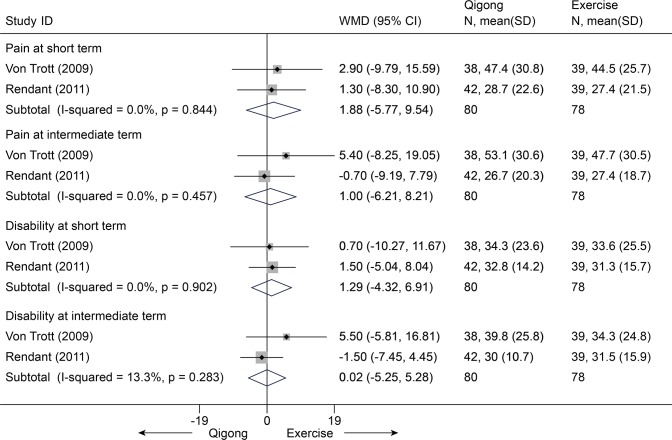
Conclusions: Acupuncture, acupressure, and cupping could be efficacious in treating the pain and disability associated with CNP or CLBP in the immediate term. Gua sha, tai chi, qigong, and Chinese manipulation showed fair effects, but we were unable to draw any definite conclusions, and further research is still needed. The efficacy of tuina and moxibustion is unknown because no direct evidence was obtained. These TCM modalities are relatively safe.
Conflict of interest statement
Figures
References
-
- Andersson G (1997) The epidemiology of spinal disorders In: Frymoyer J, editor. The adult spine: Principles and practice. Philadelphia: Lippincott-Raven.
-
- Mäkela M, Heliövaara M, Sievers K, Impivaara O, Knekt P, et al. (1991) Prevalence, determinants, and consequences of chronic neck pain in Finland. Am J Epidemiol 134: 1356–1367. - PubMed
-
- Côté P, Cassidy JD, Carroll L (1998) The Saskatchewan health and back pain survey: the prevalence of neck pain and related disability in Saskatchewan adults. Spine (Phila Pa 1976) 23: 1689–1698. - PubMed
-
- Chou R, Shekelle P (2010) Will this patient develop persistent disabling low back pain? J Am Med Assoc 303: 1295–1302. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
