

Clinical and radiographic assessment of the efficacy of calcium silicate indirect pulp capping: a randomized controlled clinical trial
- PMID: 25710953
- PMCID: PMC4485218
- DOI: 10.1177/0022034515571415
Clinical and radiographic assessment of the efficacy of calcium silicate indirect pulp capping: a randomized controlled clinical trial
Abstract
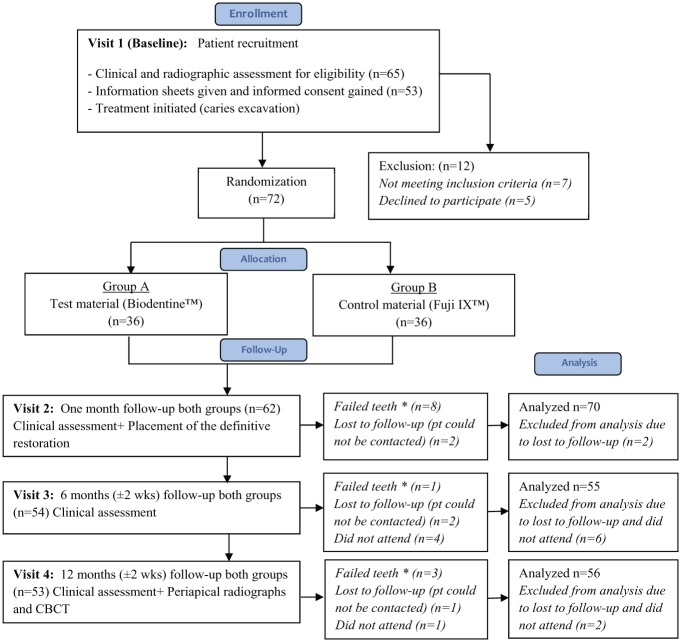
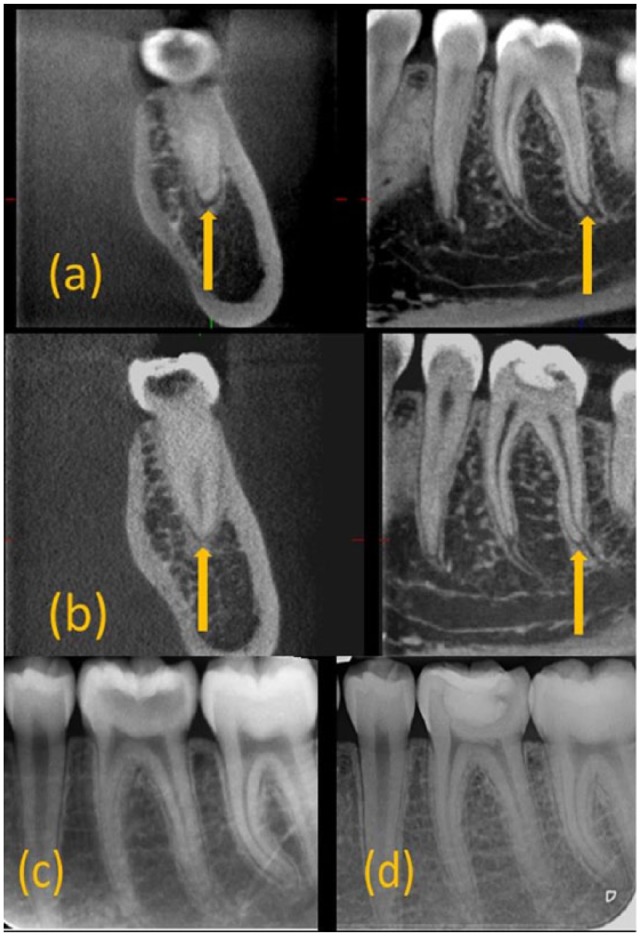
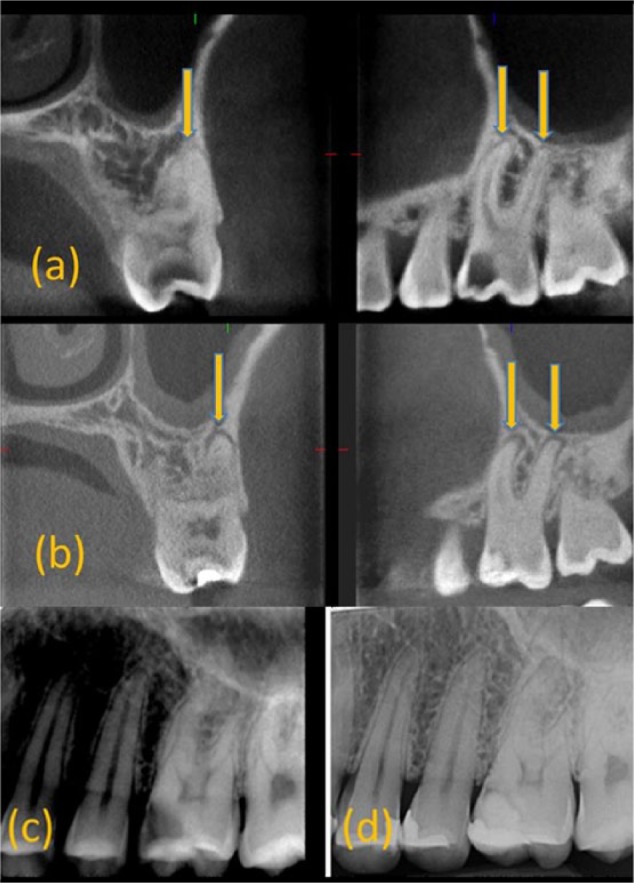
The aims of this study were to assess the effectiveness of calcium silicate cement (Biodentine) versus glass ionomer cement (GIC; control group) as indirect pulp capping materials in patients with reversible pulpitis and to compare the effectiveness of cone beam computed tomography (CBCT) versus periapical (PA) radiographs in detecting PA changes at baseline (T0) and at 12 mo (T12) postoperatively. Seventy-two restorations (36 Biodentine, 36 Fuji IX) were placed randomly in 53 patients. CBCT/PA radiographs were taken at T0 and T12. Two calibrated examiners assessed the presence/absence and increase/decrease in the size of existing PA radiolucencies under standardized conditions. The Kappa coefficient evaluated statistically the effectiveness of CBCT versus PA radiographs in detecting PA changes. Chi-square/Mann-Whitney tests were used to evaluate the association between PA changes in CBCT with various clinical measures. Significance was predetermined at α = 0.05. Clinical success rates for Biodentine and Fuji IX GIC were 83.3%. CBCT was significantly more effective in detecting PA radiolucencies compared with radiographs (P = 0.0069). Of the teeth, 65.4% and 90.4% were deemed healthy using CBCT and PA radiographs, respectively, at T12. Healing/healed rates were 17.3%/0%, while new/progressed radiolucency were 30.8%/9.6% with CBCT/PA radiographs, respectively. Seventy-one percent of healed lesions had received Biodentine; 88% of new/progressed lesions received Fuji IX GIC. Teeth presenting with an initial CBCT PA lesion had a failure rate of 63%, whereas teeth with no initial lesion had a failure rate of 16%. Although no statistically significant difference was detected in the clinical efficacy of Biodentine/Fuji IX when used as indirect pulp capping materials in patients with reversible pulpitis, CBCT showed a significant difference in that most healed CBCT lesions had received Biodentine while most that did not heal received Fuji IX. Longer-term follow-up is needed to establish their effect on the healing dynamics of PA tissues (ClinicalTrials.gov NCT02201641).
Keywords: cone beam computed tomography; dental caries; dental radiography; glass ionomer cements; periapical disease; pulpitis.
© International & American Associations for Dental Research 2015.
Conflict of interest statement
The authors declare no potential conflicts of interest with respect to the authorship and/or publication of this article.
Figures
References
-
- Aguilar P, Linsuwanont P. 2011. Vital pulp therapy in vital permanent teeth with cariously exposed pulp: a systematic review. J Endod. 37(5):581–587. - PubMed
-
- Banerjee A, Watson TF. 2011. Pickard’s manual of operative dentistry. Oxford (UK): Oxford University Press.
-
- Barthel CR, Rosenkranz B, Leuenberg A, Roulet JF. 2000. Pulp capping of carious exposures: treatment outcome after 5 and 10 years: a retrospective study. J Endod. 26(9):525–528. - PubMed
-
- Bender IB. 2000. Pulpal pain diagnosis—a review. J Endod. 26(3):175–179. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
