

Patient controlled analgesia with remifentanil versus epidural analgesia in labour: randomised multicentre equivalence trial
- PMID: 25713015
- PMCID: PMC4353278
- DOI: 10.1136/bmj.h846
Patient controlled analgesia with remifentanil versus epidural analgesia in labour: randomised multicentre equivalence trial
Abstract
Objective: To determine women's satisfaction with pain relief using patient controlled analgesia with remifentanil compared with epidural analgesia during labour.
Design: Multicentre randomised controlled equivalence trial.
Setting: 15 hospitals in the Netherlands.
Participants: Women with an intermediate to high obstetric risk with an intention to deliver vaginally. To exclude a clinically relevant difference in satisfaction with pain relief of more than 10%, we needed to include 1136 women. Because of missing values for satisfaction this number was increased to 1400 before any analysis. We used multiple imputation to correct for missing data.
Intervention: Before the onset of active labour consenting women were randomised to a pain relief strategy with patient controlled remifentanil or epidural analgesia if they requested pain relief during labour.
Main outcome measures: Primary outcome was satisfaction with pain relief, measured hourly on a visual analogue scale and expressed as area under the curve (AUC), thus providing a time weighted measure of total satisfaction with pain relief. A higher AUC represents higher satisfaction with pain relief. Secondary outcomes were pain intensity scores, mode of delivery, and maternal and neonatal outcomes. Analysis was done by intention to treat. The study was defined as an equivalence study for the primary outcome.
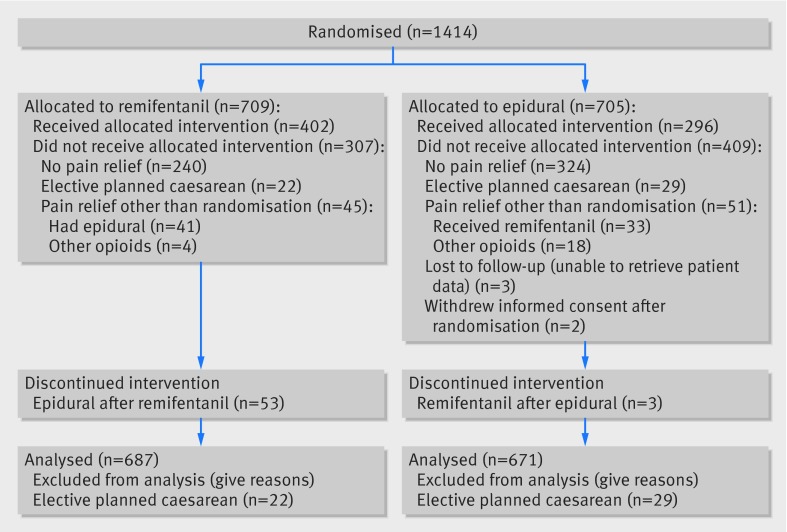
Results: 1414 women were randomised, of whom 709 were allocated to patient controlled remifentanil and 705 to epidural analgesia. Baseline characteristics were comparable. Pain relief was ultimately used in 65% (447/687) in the remifentanil group and 52% (347/671) in the epidural analgesia group (relative risk 1.32, 95% confidence interval 1.18 to 1.48). Cross over occurred in 7% (45/687) and 8% (51/671) of women, respectively. Of women primarily treated with remifentanil, 13% (53/402) converted to epidural analgesia, while in women primarily treated with epidural analgesia 1% (3/296) converted to remifentanil. The area under the curve for total satisfaction with pain relief was 30.9 in the remifentanil group versus 33.7 in the epidural analgesia group (mean difference -2.8, 95% confidence interval -6.9 to 1.3). For who actually received pain relief the area under the curve for satisfaction with pain relief after the start of pain relief was 25.6 in the remifentanil group versus 36.1 in the epidural analgesia group (mean difference -10.4, -13.9 to -7.0). The rate of caesarean section was 15% in both groups. Oxygen saturation was significantly lower (SpO2 <92%) in women who used remifentanil (relative risk 1.5, 1.4 to 1.7). Maternal and neonatal outcomes were comparable between both groups.
Conclusion: In women in labour, patient controlled analgesia with remifentanil is not equivalent to epidural analgesia with respect to scores on satisfaction with pain relief. Satisfaction with pain relief was significantly higher in women who were allocated to and received epidural analgesia.
Trial registration: Netherlands Trial Register NTR2551.
© Freeman et al 2015.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures
References
-
- NVOG (Dutch Society of Obstetrics and Gynaecology). Guideline Pijnstilling tijdens de bevalling [pain relief during labour]. NVOG, 2008.
-
- Douma MR, Verwey RA, Kam-Endtz CE, van der Linden PD, Stienstra R. Obstetric analgesia: a comparison of patient-controlled meperidine, remifentanil, and fentanyl in labor. Br J Anaesth 2010;104:209-15. - PubMed
-
- Michelsen LG, Hug CC Jr. The pharmacokinetics of remifentanil. J Clin Anesth 1996;8:679-82 - PubMed
-
- Kan RE, Hughes SC, Rosen MA, Kessin C, Preston PG, Lobo EP. Intravenous remifentanil. Anaesthesiology 1998;88:1467-749 - PubMed
-
- Volmanen P, Sarvela J, Akural EI, Raudaskoski T, Korttila K, Alahuhta S. Intravenous remifentanil vs. epidural levobupivacaine with fentanyl for pain relief in early labour: a randomised, controlled, double-blinded study. Acta Anaesthesiol Scand 2008;52:249-55 - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources