

β-Adrenergic stimulation and rapid pacing mutually promote heterogeneous electrical failure and ventricular fibrillation in the globally ischemic heart
- PMID: 25713306
- PMCID: PMC4551128
- DOI: 10.1152/ajpheart.00768.2014
β-Adrenergic stimulation and rapid pacing mutually promote heterogeneous electrical failure and ventricular fibrillation in the globally ischemic heart
Abstract
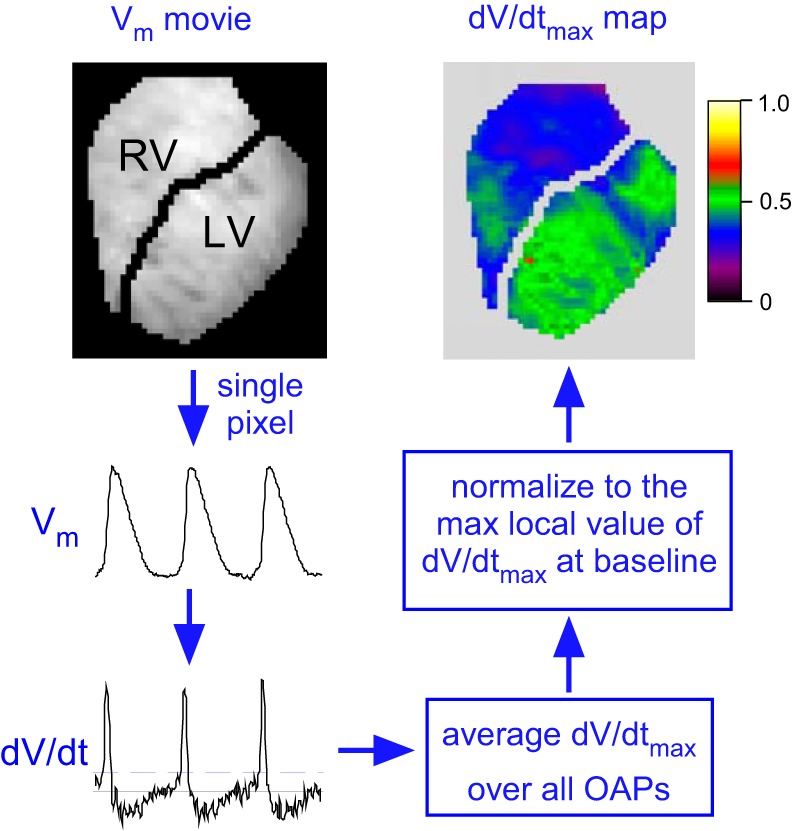
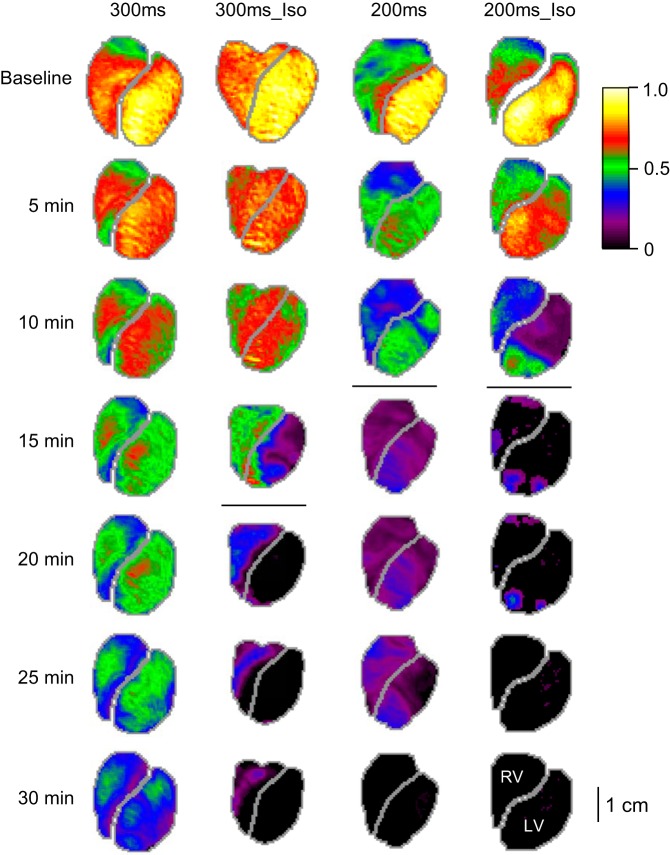
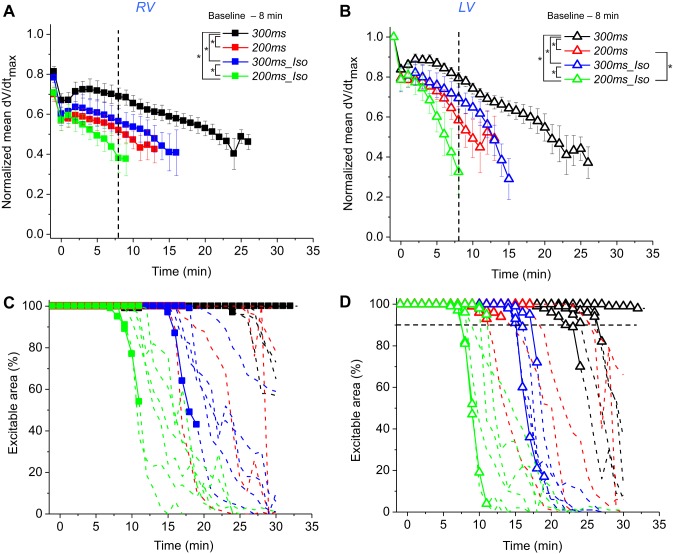
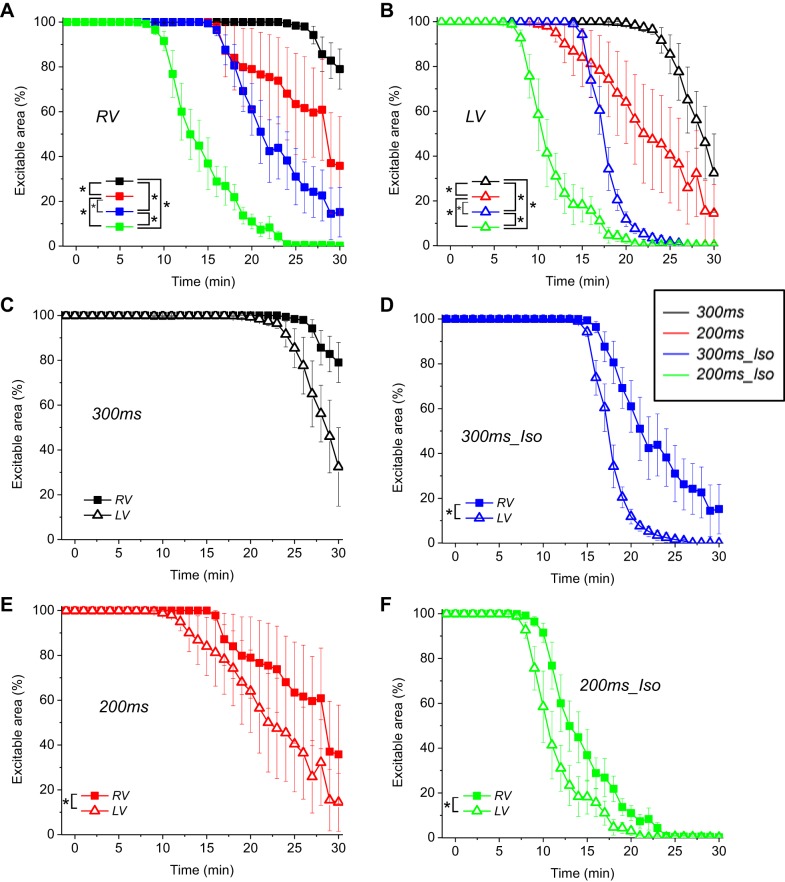
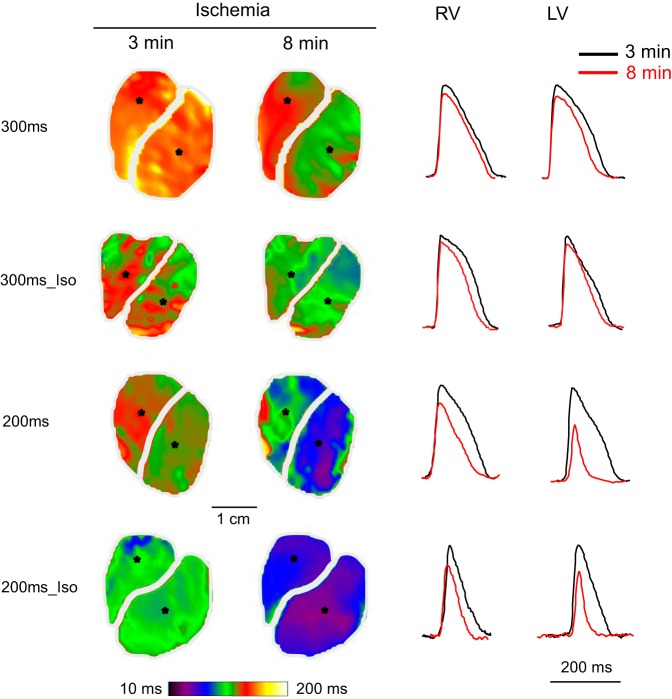
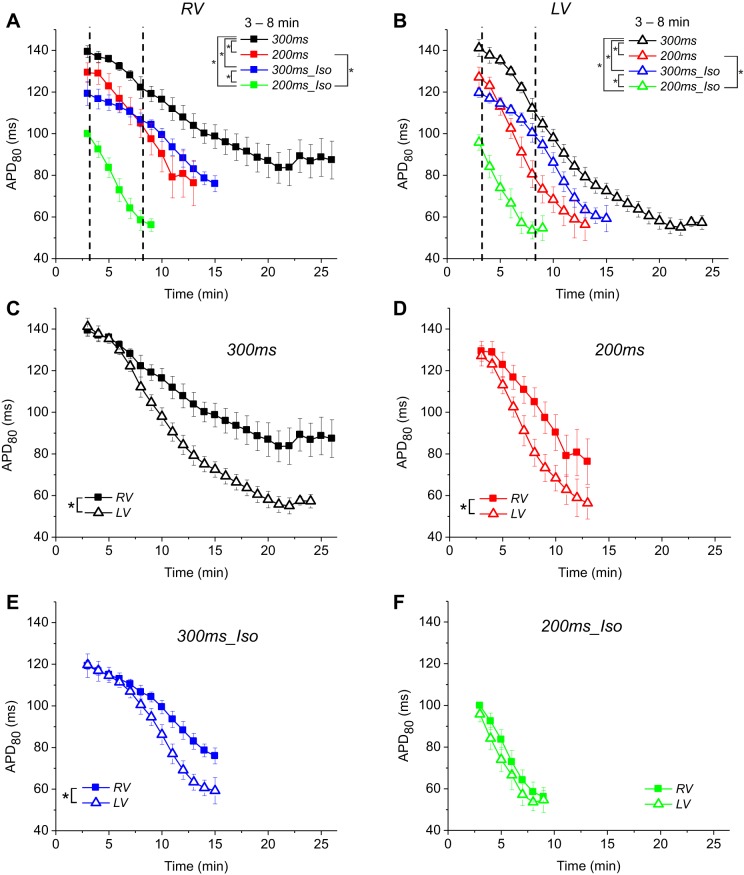
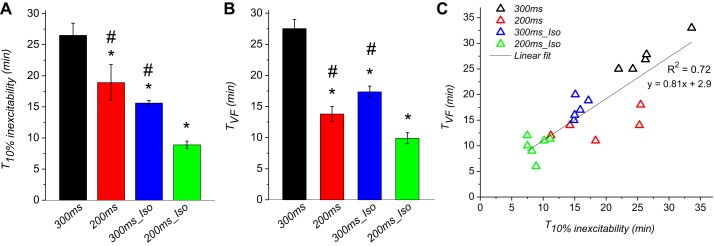
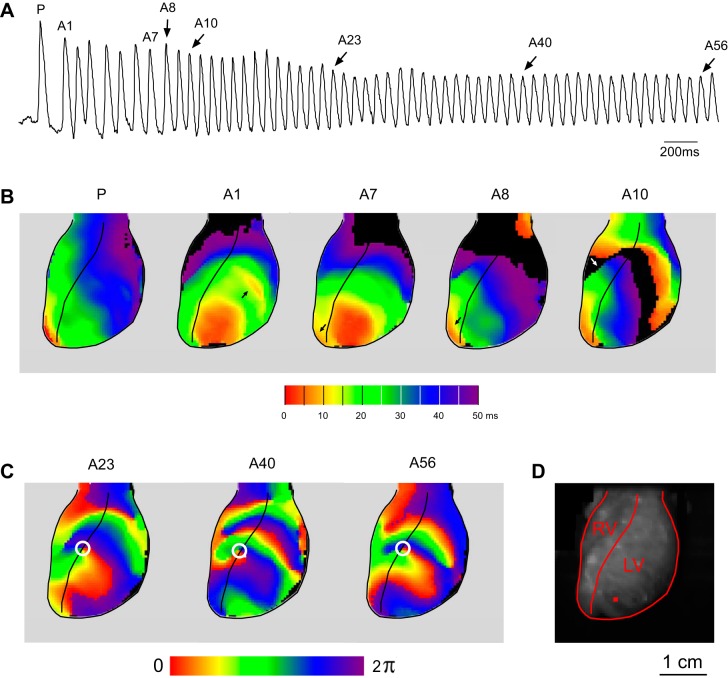
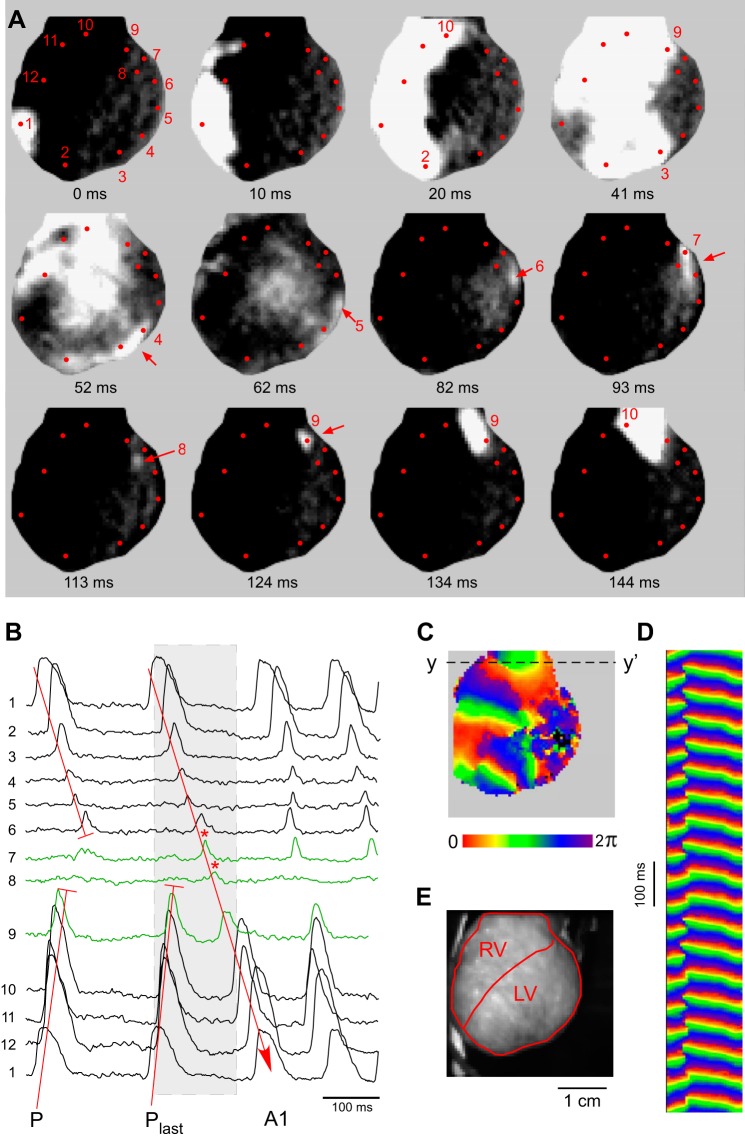
Global ischemia, catecholamine surge, and rapid heart rhythm (RHR) due to ventricular tachycardia or ventricular fibrillation (VF) are the three major factors of sudden cardiac arrest (SCA). Loss of excitability culminating in global electrical failure (asystole) is the major adverse outcome of SCA with increasing prevalence worldwide. The roles of catecholamines and RHR in the electrical failure during SCA remain unclear. We hypothesized that both β-adrenergic stimulation (βAS) and RHR accelerate electrical failure in the globally ischemic heart. We performed optical mapping of the action potential (OAP) in the right ventricular (RV) and left (LV) ventricular epicardium of isolated rabbit hearts subjected to 30-min global ischemia. Hearts were paced at a cycle length of either 300 or 200 ms, and either in the presence or in the absence of β-agonist isoproterenol (30 nM). 2,3-Butanedione monoxime (20 mM) was used to reduce motion artifact. We found that RHR and βAS synergistically accelerated the decline of the OAP upstroke velocity and the progressive expansion of inexcitable regions. Under all conditions, inexcitability developed faster in the LV than in the RV. At the same time, both RHR and βAS shortened the time to VF (TVF) during ischemia. Moreover, the time at which 10% of the mapped LV area became inexcitable strongly correlated with TVF (R(2) = 0 .72, P < 0.0001). We conclude that both βAS and RHR are major factors of electrical depression and failure in the globally ischemic heart and may contribute to adverse outcomes of SCA such as asystole and recurrent/persistent VF.
Keywords: inexcitability; myocardial ischemia; optical mapping; ventricular fibrillation; β-adrenergic stimulation.
Copyright © 2015 the American Physiological Society.
Figures
Comment in
-
Racing to the flatline: heart rate and β-adrenergic stimulation quicken the pace.Am J Physiol Heart Circ Physiol. 2015 May 1;308(9):H977-9. doi: 10.1152/ajpheart.00154.2015. Epub 2015 Mar 13. Am J Physiol Heart Circ Physiol. 2015. PMID: 25770239 Free PMC article. No abstract available.
References
-
- Aupetit JF, Frassati D, Bui-Xuan B, Freysz M, Faucon G, Timour Q. Efficacy of a β-adrenergic receptor antagonist, propranolol, in preventing ischaemic ventricular fibrillation: dependence on heart rate and ischaemia duration. Cardiovasc Res 37: 646–655, 1998. - PubMed
-
- Aupetit JF, Timour Q, Freysz M, Loufoua-Moundanga J, Omar S, Chevrel G, Faucon G. Vulnerability to ventricular fibrillation related to ischaemia: comparison of the acute effects of beta-blockers and calcium antagonists. Arch Int Pharmacodyn Ther 327: 25–39, 1994. - PubMed
-
- Bayes de Luna A, Elosua R. Sudden death. Rev Esp Cardiol 65: 1039–1052, 2012. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical