

Tracheoesophageal fistula--a complication of prolonged tracheal intubation
- PMID: 25713612
- PMCID: PMC4316129
Tracheoesophageal fistula--a complication of prolonged tracheal intubation
Abstract
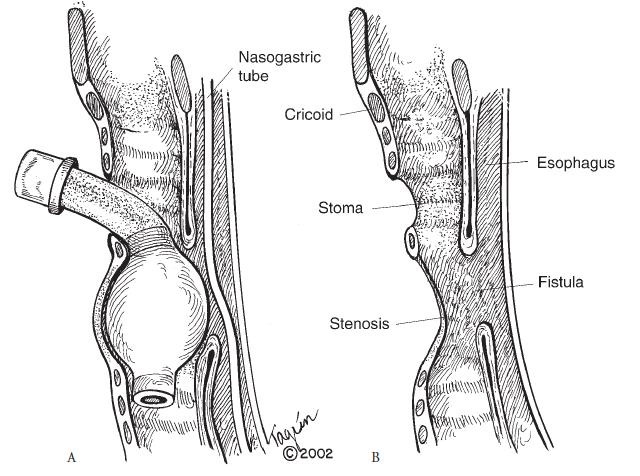
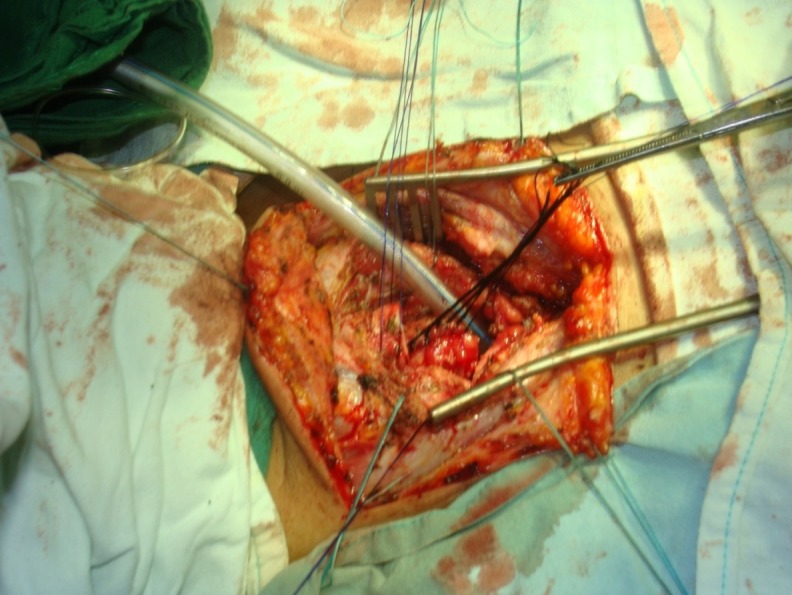
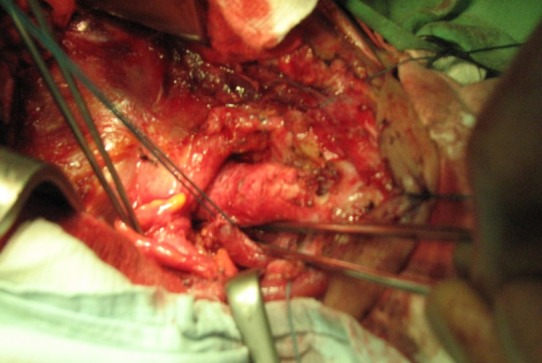
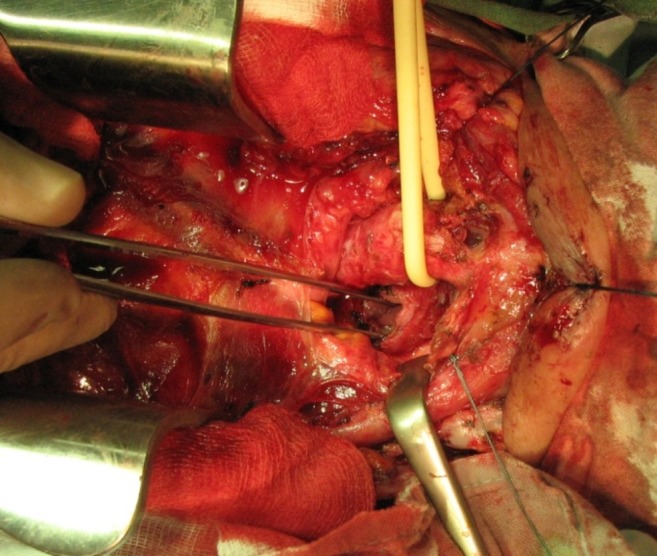
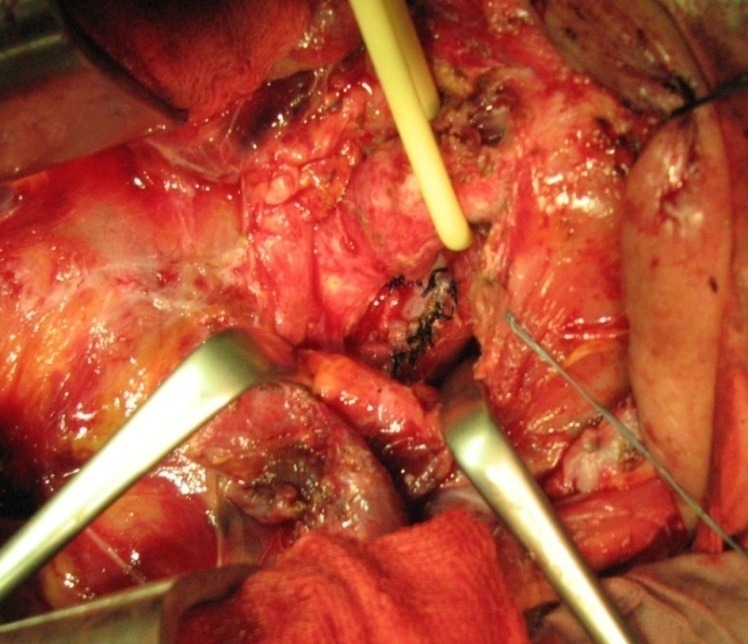
Tracheoesophageal fistula most commonly occurs as a complication of prolonged tracheal intubation. The incidence decreased after the use of low pressure and high volume endotracheal cuffs, but the intensive care units continue to provide such cases. The abnormal tracheoesophageal communication causes pulmonary contamination (with severe suppuration) and impossibility to feed the patient. The prognosis is reserved, because most patients are debilitated and ventilator dependent, with severe neurological and cardiovascular diseases. The therapeutic options are elected based on respiratory, neurological and nutritional status. The aim of conservative treatment is to stop the contamination (drainage gastrostomy, feeding jejunostomy) and to treat the pulmonary infection and biological deficits. Endoscopic therapies can be tried in cases with surgical contraindication. Operation is addressed to selected cases and consists in the dissolution of the fistula, esophageal suture with or without segmental tracheal resection associated. Esophageal diversion is rarely required. The correct indication and timing of surgery, proper surgical technique and postoperative care are prerequisites for adequate results.
Keywords: conservative treatment; prolonged tracheal intubation; surgical treatment; trachea-esophageal fistula.
Figures
Similar articles
-
Post-Intubation Tracheoesophageal Fistula: Surgical Management by Complete Cervical Tracheal Transection.Ann Thorac Cardiovasc Surg. 2024 Jan 26;30(1):22-00134. doi: 10.5761/atcs.cr.22-00134. Epub 2022 Oct 29. Ann Thorac Cardiovasc Surg. 2024. PMID: 36310067 Free PMC article.
-
A Modified Tracheal Transaction Approach for the Repair of Nonmalignant Tracheoesophageal Fistulas: A Report of 5 Cases.ORL J Otorhinolaryngol Relat Spec. 2017;79(3):147-152. doi: 10.1159/000468943. Epub 2017 Apr 8. ORL J Otorhinolaryngol Relat Spec. 2017. PMID: 28391268
-
Tracheal rupture in burns--a retrospective study.Burns. 2008 Jun;34(4):525-30. doi: 10.1016/j.burns.2007.06.017. Epub 2007 Oct 24. Burns. 2008. PMID: 17928154
-
Tracheoesophageal fistula.Chest Surg Clin N Am. 2003 May;13(2):271-89. doi: 10.1016/s1052-3359(03)00030-9. Chest Surg Clin N Am. 2003. PMID: 12755313 Review.
-
Surgical approach for iatrogenic tracheoesophageal fistula. Case report and literature review.Cir Cir. 2021;89(6):811-817. doi: 10.24875/CIRU.20000730. Cir Cir. 2021. PMID: 34851590 Review. English.
Cited by
-
Airway and anesthesia management in tracheoesophageal fistula closure implantation: a single-centre retrospective study.J Cardiothorac Surg. 2024 Apr 3;19(1):172. doi: 10.1186/s13019-024-02737-4. J Cardiothorac Surg. 2024. PMID: 38570837 Free PMC article.
-
Direct and indirect CT imaging features of esophago-airway fistula in adults.J Thorac Dis. 2020 Jun;12(6):3157-3166. doi: 10.21037/jtd-20-244. J Thorac Dis. 2020. PMID: 32642237 Free PMC article.
-
Efficacy and Safety of Endoscopic Esophageal Dilatation in Pediatric Patients with Esophageal Strictures.Int J Pediatr. 2021 Sep 24;2021:1277530. doi: 10.1155/2021/1277530. eCollection 2021. Int J Pediatr. 2021. PMID: 34608394 Free PMC article.
-
Tracheoesophageal Fistulas Unrelated to Malignancy: A Case Series.Cureus. 2025 May 22;17(5):e84605. doi: 10.7759/cureus.84605. eCollection 2025 May. Cureus. 2025. PMID: 40546474 Free PMC article.
-
Prolonged Intubation Induced Tracheoesophageal Fistula in Suspected Meningococcal Sepsis with ARDS: A Case Report.JNMA J Nepal Med Assoc. 2018 Nov-Dec;56(214):980-982. doi: 10.31729/jnma.3890. JNMA J Nepal Med Assoc. 2018. PMID: 31065149 Free PMC article.
References
-
- Couraud L, Bercovici D, Zanotti L, et al. Traitment often fistules oesophago - trachéales from réanimation. Ann Chir Thorac Cardiovasc. 1989;43:677–681. - PubMed
-
- Marcelle J, Dartevelle P, Khalife J, et al. Surgical Management of Acquired tracheoesophageal fistulas postintubation 27 Patients. Eur J Cardiothoracic Surg. 1989;3:499–503. - PubMed
-
- Galan G, Tarrazona V, Soliveres J, Calvo V, Paris F. Tracheoplasty in a large tracheoesophageal fistula. Thorac Surg. 1999;68:1071–1072. - PubMed
-
- Couraud L, Ballester ML. Tracheoesophageal fistula Delaisement C. Acquired and STI management. Semin Thorac Cardiovasc Surg. 1998;8:392–399. - PubMed
-
- Payne DK, Anderson WM, Romero MD, Wissing DR, Fowler M. Tracheoesophageal fistula formation in intubated Patients. Chest. 1990;98:161–164. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources