

Recurrence of papillary thyroid cancer after optimized surgery
- PMID: 25713780
- PMCID: PMC4321046
- DOI: 10.3978/j.issn.2227-684X.2014.12.06
Recurrence of papillary thyroid cancer after optimized surgery
Abstract
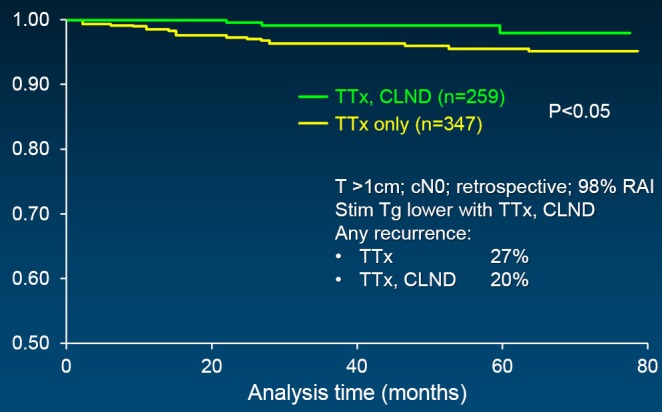
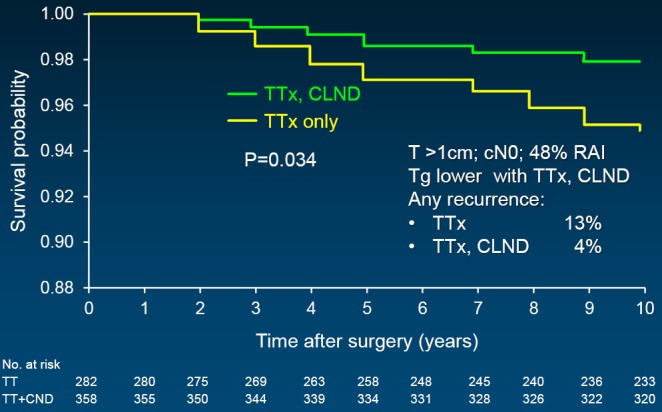
Recurrence of papillary thyroid cancer (PTC) after optimized surgery requires a full understanding of the disease, especially as it has changed in the last 15 years, what comprises optimized surgery, and the different types and implications of disease relapse that can be encountered. PTC has evolved to tumors that are much smaller than previously seen, largely due to various high quality imaging studies obtained for different reasons, but serendipitously identifying thyroid nodules that prove to be papillary thyroid microcarcinomas (PTMC). With rare exception, these cancers are cured by conservative surgery without additional therapy, and seldom result in recurrent disease. PTC is highly curable in 85% of cases because of its rather innocent biologic behavior. Therefore, the shift in emphasis from disease survival to recurrence is appropriate. As a result of three technologic advances-high-resolution ultrasound (US), recombinant TSH, and highly sensitive thyroglobulin (Tg)-disease relapse can be discovered when it is subclinical. Endocrinologists who largely control administration of radioactive iodine have used it to ablate barely detectable or even biochemically apparent disease, hoping to reduce recurrence and perhaps improve survival. Surgeons, in response to this new intense postoperative surveillance that has uncovered very small volume disease, have responded by utilizing US preoperatively to image this disease, and incorporated varying degrees of lymphadenectomy into their initial treatment algorithm. Bilateral thyroid resection-either total or near-total thyroidectomy-remains the standard for PTC >1 cm, although recent data has re-emphasized the value of unilateral lobectomy in treating even some PTC measuring 1-4 cm. Therapeutic lymphadenectomy has universal approval, but when lymph nodes in the central neck are not worrisome to the surgeon's intraoperative assessment, although that judgment in incorrect up to 50%, whether they should be excised has reached a central point of controversy. Disease relapse can occur individually or in combination of three different forms: lymph node metastasis (LNM), true soft tissue local recurrence, and distant disease. The latter two are worrisome for potentially life-threatening consequences whereas nodal metastases are often persistent from the initial operation, and mostly comprise a biologic nuisance rather than virulent disease. A moderate surgical approach of bilateral thyroid resection, with usual central neck nodal clearance, and lateral internal jugular lymphadenectomy for node-positive disease can be performed safely, and with about a 5% recurrence rate.
Keywords: Papillary thyroid cancer (PTC); lymph nodes; recurrence; surgery.
Figures
References
-
- Davies L, Welch HG. Increasing incidence of thyroid cancer in the United States, 1973-2002. JAMA 2006;295:2164-7. - PubMed
-
- Hughes DT, Haymart MR, Miller BS, et al. The most commonly occurring papillary thyroid cancer in the United States is now a microcarcinoma in a patient older than 45 years. Thyroid 2011;21:231-6. - PubMed
-
- Harach HR, Franssila KO, Wasenius VM. Occult papillary carcinoma of the thyroid. A "normal" finding in Finland. A systematic autopsy study. Cancer 1985;56:531-8. - PubMed
-
- Lang W, Borrusch H, Bauer L.Occult carcinomas of the thyroid. Evaluation of 1,020 sequential autopsies. Am J Clin Pathol 1988;90:72-6. - PubMed
-
- Ito Y, Uruno T, Nakano K, et al. An observation trial without surgical treatment in patients with papillary microcarcinoma of the thyroid. Thyroid 2003;13:381-7. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous