

Community-acquired pneumonia requiring hospitalization among U.S. children
- PMID: 25714161
- PMCID: PMC4697461
- DOI: 10.1056/NEJMoa1405870
Community-acquired pneumonia requiring hospitalization among U.S. children
Abstract
Background: Incidence estimates of hospitalizations for community-acquired pneumonia among children in the United States that are based on prospective data collection are limited. Updated estimates of pneumonia that has been confirmed radiographically and with the use of current laboratory diagnostic tests are needed.
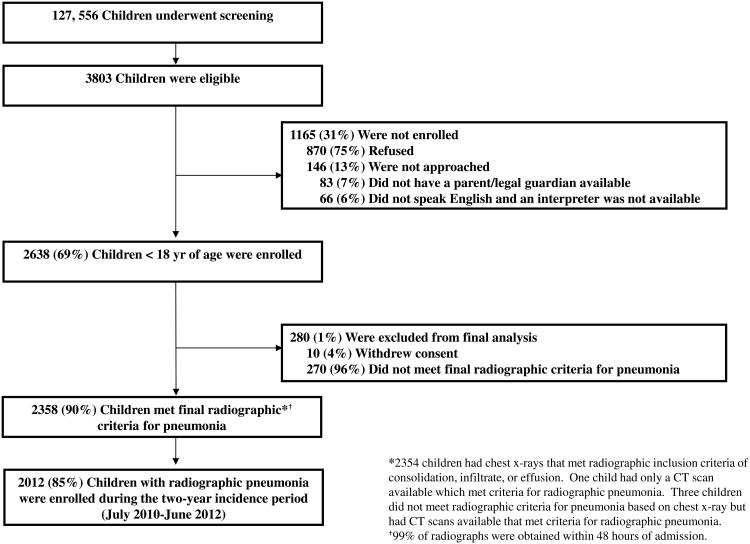
Methods: We conducted active population-based surveillance for community-acquired pneumonia requiring hospitalization among children younger than 18 years of age in three hospitals in Memphis, Nashville, and Salt Lake City. We excluded children with recent hospitalization or severe immunosuppression. Blood and respiratory specimens were systematically collected for pathogen detection with the use of multiple methods. Chest radiographs were reviewed independently by study radiologists.
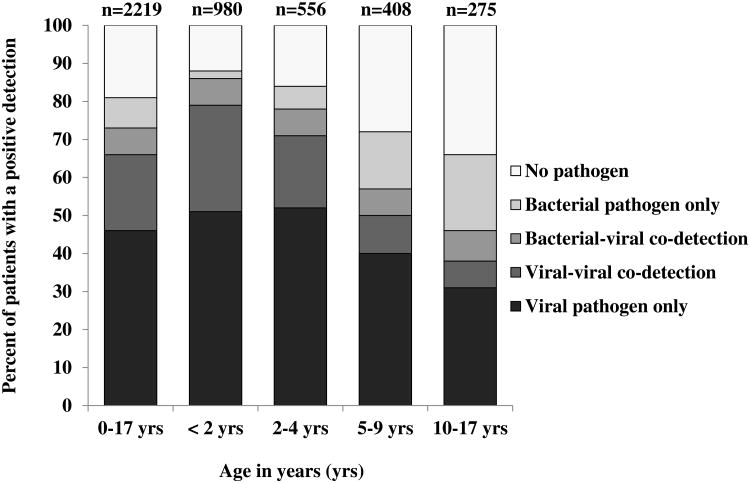
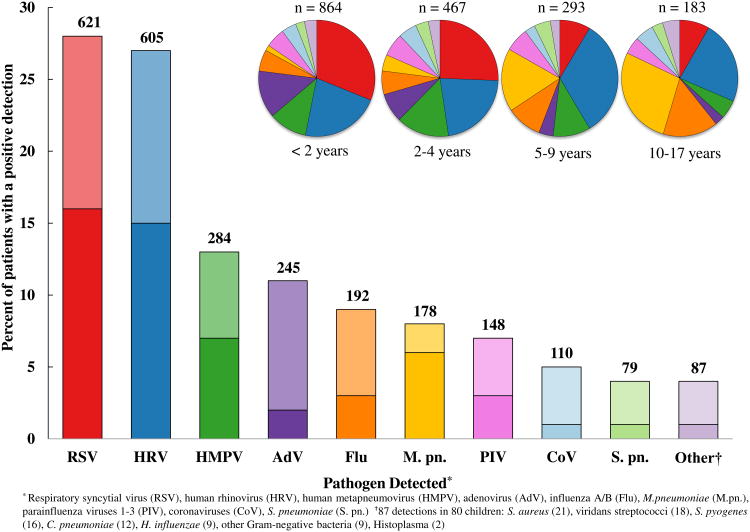
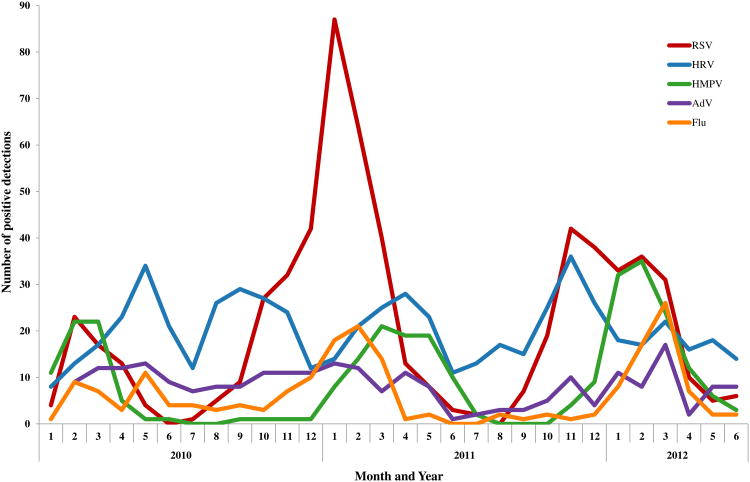
Results: From January 2010 through June 2012, we enrolled 2638 of 3803 eligible children (69%), 2358 of whom (89%) had radiographic evidence of pneumonia. The median age of the children was 2 years (interquartile range, 1 to 6); 497 of 2358 children (21%) required intensive care, and 3 (<1%) died. Among 2222 children with radiographic evidence of pneumonia and with specimens available for bacterial and viral testing, a viral or bacterial pathogen was detected in 1802 (81%), one or more viruses in 1472 (66%), bacteria in 175 (8%), and both bacterial and viral pathogens in 155 (7%). The annual incidence of pneumonia was 15.7 cases per 10,000 children (95% confidence interval [CI], 14.9 to 16.5), with the highest rate among children younger than 2 years of age (62.2 cases per 10,000 children; 95% CI, 57.6 to 67.1). Respiratory syncytial virus was more common among children younger than 5 years of age than among older children (37% vs. 8%), as were adenovirus (15% vs. 3%) and human metapneumovirus (15% vs. 8%). Mycoplasma pneumoniae was more common among children 5 years of age or older than among younger children (19% vs. 3%).
Conclusions: The burden of hospitalization for children with community-acquired pneumonia was highest among the very young, with respiratory viruses the most commonly detected causes of pneumonia. (Funded by the Influenza Division of the National Center for Immunization and Respiratory Diseases.).
Figures
Comment in
-
Community-acquired pneumonia among U.S. children.N Engl J Med. 2015 May 28;372(22):2167-8. doi: 10.1056/NEJMc1504028. N Engl J Med. 2015. PMID: 26017833 Free PMC article. No abstract available.
-
Community-acquired pneumonia among U.S. children.N Engl J Med. 2015 May 28;372(22):2166-7. doi: 10.1056/NEJMc1504028. N Engl J Med. 2015. PMID: 26017834 No abstract available.
-
Community-acquired pneumonia among U.S. children.N Engl J Med. 2015 May 28;372(22):2167. doi: 10.1056/NEJMc1504028. N Engl J Med. 2015. PMID: 26017835 No abstract available.
References
-
- Pfuntner A, Wier LM, Stocks C. Rockville, Md.: Agency for Healthcare Research and Quality; 2013. [February 10, 2014]. Most frequent conditions in U.S. hospitals, 2011. HCUP Statistical Brief #162. at http://www.hcup-us.ahrq.gov/reports/statbriefs/sb162.pdf. - PubMed
-
- Yu H, Wier LM, Elixhauser A. Rockville, Md.: Agency for Healthcare Research and Quality; 2011. [February 10, 2014]. Hospital stays for children, 2009. HCUP Statistical Brief #118. at http://www.hcup-us.ahrq.gov/reports/statbriefs/sb118.pdf. - PubMed
-
- Pfuntner A, Wier LM, Steiner C. Rockville, Md.: Agency for Healthcare Research and Quality; 2013. [April 21, 2014]. Costs for Hospital Stays in the United States, 2011. HCUP Statistical Brief #168. at http://www.hcup-us.ahrq.gov/reports/statbriefs/sb168-Hospital-Costs-Unit.... - PubMed
-
- Bradley JS, Byington CL, Shah SS, et al. The management of community-acquired pneumonia in infants and children older than 3 months of age: clinical practice guidelines by the Pediatric Infectious Diseases Society and the Infectious Diseases Society of America. Clin Infect Dis. 2011;53:617–30. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical