

Comparative effectiveness of different forms of telemedicine for individuals with heart failure (HF): a systematic review and network meta-analysis
- PMID: 25714962
- PMCID: PMC4340962
- DOI: 10.1371/journal.pone.0118681
Comparative effectiveness of different forms of telemedicine for individuals with heart failure (HF): a systematic review and network meta-analysis
Abstract
Background: Previous studies on telemedicine have either focused on its role in the management of chronic diseases in general or examined its effectiveness in comparison to standard post-discharge care. Little has been done to determine the comparative impact of different telemedicine options for a specific population such as individuals with heart failure (HF).
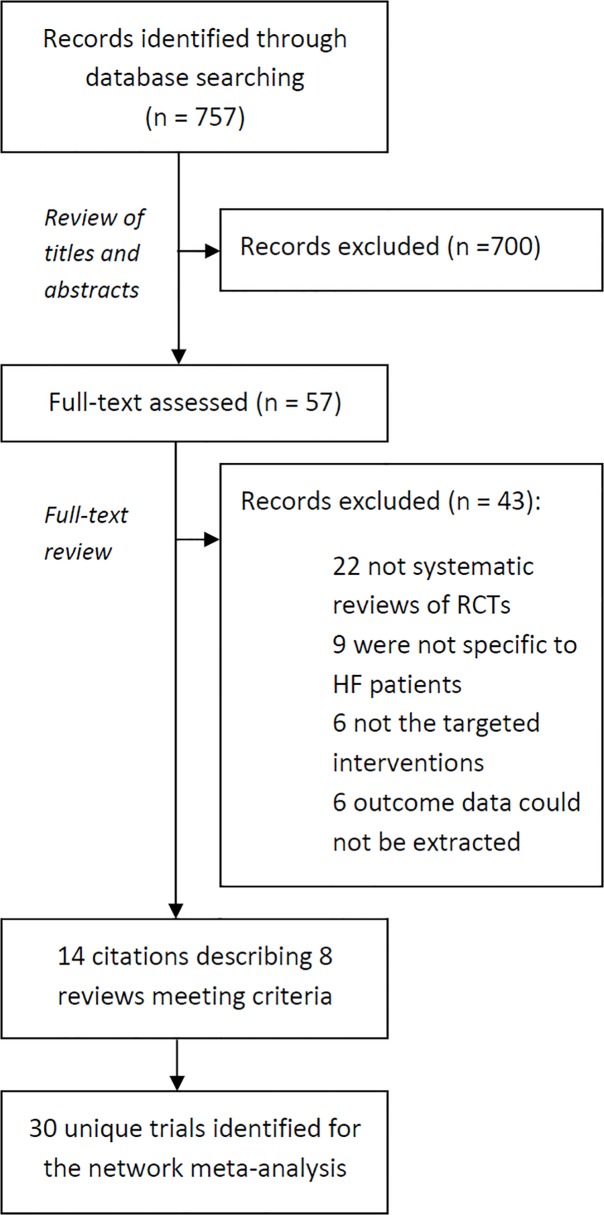
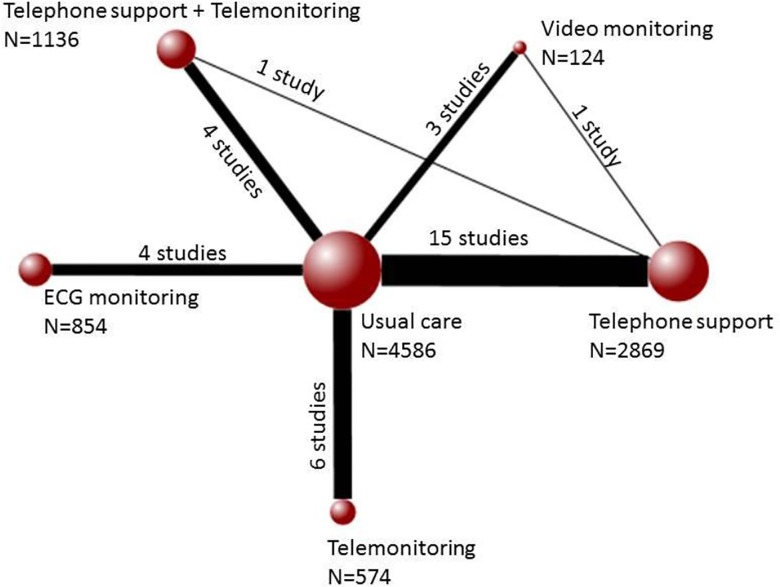
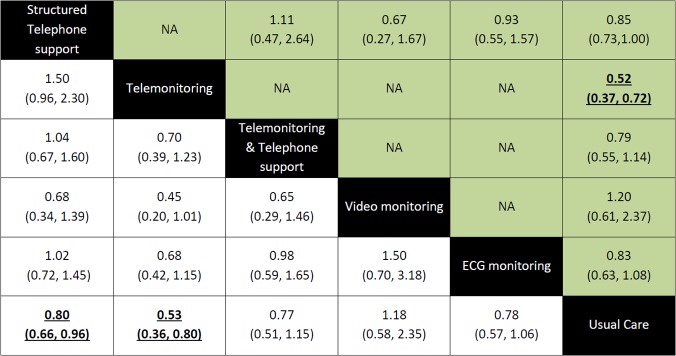
Methods and findings: Systematic reviews (SR) of randomized controlled trials (RCTs) that examined telephone support, telemonitoring, video monitoring or electrocardiographic monitoring for HF patients were identified using a comprehensive search of the following databases: MEDLINE, EMBASE, CINAHL and The Cochrane Library. Studies were included if they reported the primary outcome of mortality or any of the following secondary outcomes: all-cause hospitalization and heart failure hospitalization. Thirty RCTs (N = 10,193 patients) were included. Compared to usual care, structured telephone support was found to reduce the odds of mortality(Odds Ratio 0.80; 95% Credible Intervals [0.66 to 0.96]) and hospitalizations due to heart failure (0.69; [0.56 to 0.85]). Telemonitoring was also found to reduce the odds of mortality(0.53; [0.36 to 0.80]) and reduce hospitalizations related to heart failure (0.64; [0.39 to 0.95]) compared to usual post-discharge care. Interventions that involved ECG monitoring also reduced the odds of hospitalization due to heart failure (0.71; [0.52 to 0.98]).
Limitations: Much of the evidence currently available has focused on the comparing either telephone support or telemonitoring with usual care. This has therefore limited our current understanding of how some of the less common forms of telemedicine compare to one another.
Conclusions: Compared to usual care, structured telephone support and telemonitoring significantly reduced the odds of deaths and hospitalization due to heart failure. Despite being the most widely studied forms of telemedicine, little has been done to directly compare these two interventions against one another. Further research into their comparative cost-effectiveness is also warranted.
Conflict of interest statement
Figures
References
-
- Inglis SC, Clark RA, McAlister FA, Ball J, Lewinter C, Cullington D, et al. Structured telephone support or telemonitoring programmes for patients with chronic heart failure. Cochrane database of systematic reviews. 2011; 6. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
