

Portal hypertension induced by congenital hepatic arterioportal fistula: report of four clinical cases and review of the literature
- PMID: 25717263
- PMCID: PMC4326165
- DOI: 10.3748/wjg.v21.i7.2229
Portal hypertension induced by congenital hepatic arterioportal fistula: report of four clinical cases and review of the literature
Abstract
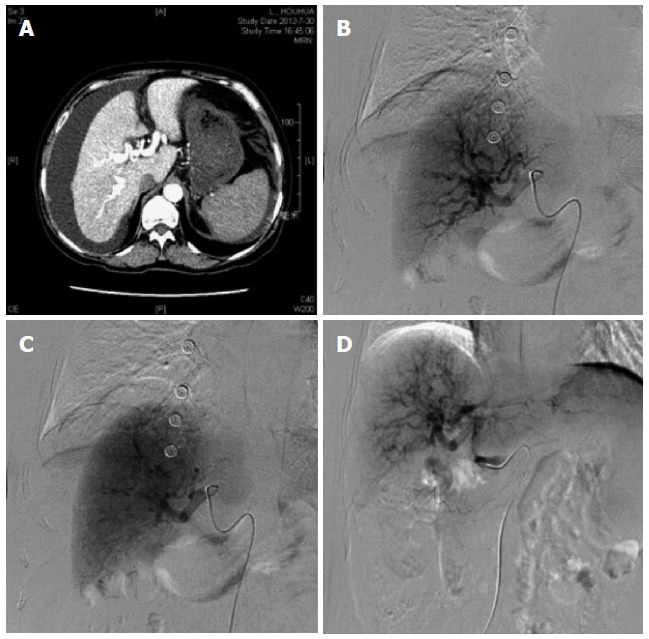
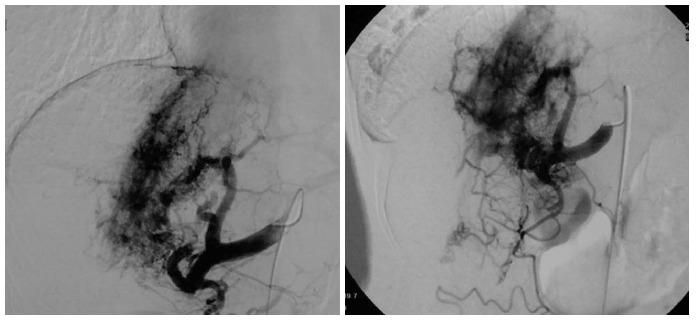
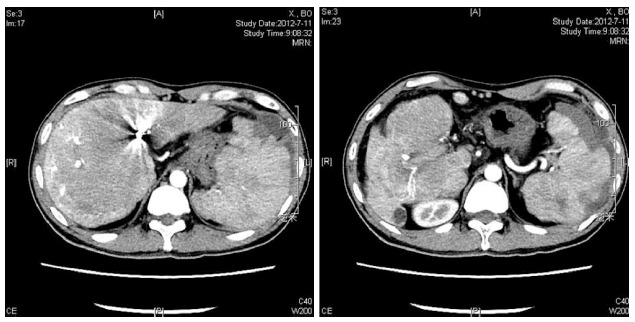
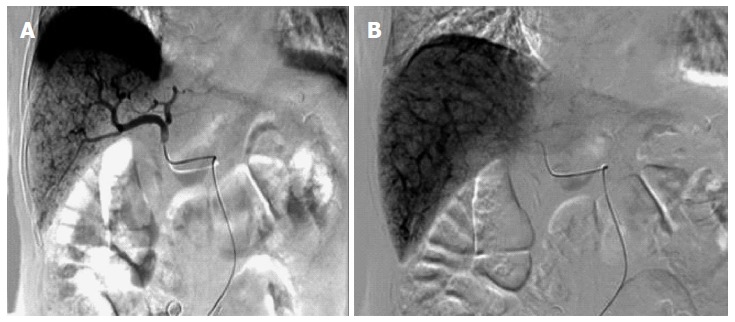
Intrahepatic arterioportal fistula (IAPF) can be caused by many secondary factors. We report four cases of portal hypertension that were eventually determined to be caused by congenital hepatic arterioportal fistula. The clinical manifestations included ascites, variceal hemorrhage and hepatic encephalopathy. Computed tomography scans from all of the patients revealed the early enhancement of the portal branches in the hepatic arterial phase. All patients were diagnosed using digital subtraction angiography (DSA). DSA before embolization revealed an arteriovenous fistula with immediate filling of the portal venous radicles. All four patients were treated with interventional embolization. The four patients remained in good condition throughout follow-up and at the time of publication. IAPF is frequently misdiagnosed due to its rarity; therefore, clinicians should consider IAPF as a potential cause of non-cirrhotic portal hypertension.
Keywords: Ascites; Intrahepatic arterioportal fistula; Portal hypertension.
Figures
Similar articles
-
Isolated arterioportal fistula presenting with variceal hemorrhage.World J Gastroenterol. 2013 May 7;19(17):2714-7. doi: 10.3748/wjg.v19.i17.2714. World J Gastroenterol. 2013. PMID: 23674881 Free PMC article.
-
The congenital intrahepatic arterioportal fistula syndrome: elucidation and proposed classification.J Pediatr Gastroenterol Nutr. 2006 Aug;43(2):248-55. doi: 10.1097/01.mpg.0000221890.13630.ad. J Pediatr Gastroenterol Nutr. 2006. PMID: 16877994 Review.
-
Coil embolization of a solitary congenital intrahepatic hepatoportal fistula.Abdom Imaging. 2001 Mar-Apr;26(2):194-6. doi: 10.1007/s002610000116. Abdom Imaging. 2001. PMID: 11178699
-
Unusual case of digestive hemorrhage: celiac axis-portal vein arteriovenous fistula.World J Gastroenterol. 2015 Jan 28;21(4):1362-4. doi: 10.3748/wjg.v21.i4.1362. World J Gastroenterol. 2015. PMID: 25632214 Free PMC article.
-
Intrahepatic spontaneous arterioportal fistula: duplex ultrasound diagnosis and angiographic treatment.Am J Gastroenterol. 1991 Jun;86(6):775-8. Am J Gastroenterol. 1991. PMID: 2039006 Review.
Cited by
-
Congenital Visceral Vascular Variation Causing Gastrointestinal Hemorrhage: A Case Report.Front Pediatr. 2021 Nov 18;9:772529. doi: 10.3389/fped.2021.772529. eCollection 2021. Front Pediatr. 2021. PMID: 34869125 Free PMC article.
-
Transarterial and Transhepatic Endovascular Intervention to Alleviate Portal Hypertension Secondary to Arterioportal Fistula in a Trisomy 21 Infant.J Pediatr Intensive Care. 2018 Mar;7(1):54-58. doi: 10.1055/s-0037-1603822. Epub 2017 Jun 21. J Pediatr Intensive Care. 2018. PMID: 31073469 Free PMC article.
-
Case report: Congenital arterioportal fistula: An unusual cause of variceal bleeding in adults.Front Med (Lausanne). 2022 Sep 7;9:970254. doi: 10.3389/fmed.2022.970254. eCollection 2022. Front Med (Lausanne). 2022. PMID: 36160178 Free PMC article.
-
Arterial-portal fistula treated with hepatic arterial embolization and portal venous aneurysm stent-graft exclusion complicated by type 2 endoleak.Radiol Case Rep. 2019 Aug 20;14(10):1301-1305. doi: 10.1016/j.radcr.2019.08.005. eCollection 2019 Oct. Radiol Case Rep. 2019. PMID: 31467626 Free PMC article.
-
A traumatic hepatic artery pseudoaneurysm and arterioportal fistula, with severe diarrhea as the first symptom: A case report and review of the literature.Medicine (Baltimore). 2018 Feb;97(7):e9893. doi: 10.1097/MD.0000000000009893. Medicine (Baltimore). 2018. PMID: 29443759 Free PMC article.
References
-
- García-Pagán JC, Gracia-Sancho J, Bosch J. Functional aspects on the pathophysiology of portal hypertension in cirrhosis. J Hepatol. 2012;57:458–461. - PubMed
-
- Berzigotti A, Seijo S, Reverter E, Bosch J. Assessing portal hypertension in liver diseases. Expert Rev Gastroenterol Hepatol. 2013;7:141–155. - PubMed
-
- Khanna R, Sarin SK. Non-cirrhotic portal hypertension - diagnosis and management. J Hepatol. 2014;60:421–441. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
