

Neuromuscular blockade improves first-attempt success for intubation in the intensive care unit. A propensity matched analysis
- PMID: 25719512
- PMCID: PMC5466156
- DOI: 10.1513/AnnalsATS.201411-517OC
Neuromuscular blockade improves first-attempt success for intubation in the intensive care unit. A propensity matched analysis
Abstract
Rationale: The use of neuromuscular blocking agents (NMBAs) has been shown to be valuable in improving successful tracheal intubation in the operating room and emergency department. However, data on NMBA use in critically ill intensive care unit (ICU) patients are lacking. Furthermore, there are no data on NMBA use with video laryngoscopy.
Objectives: To evaluate the effect of NMBA use on first-attempt success (FAS) with tracheal intubation in the ICU.
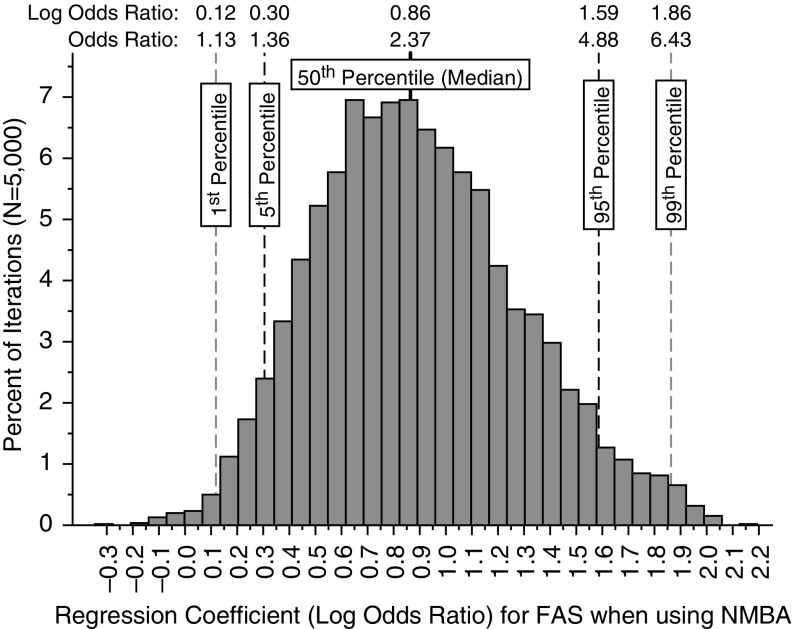
Methods: Single-center observational study of 709 consecutive patients intubated in the medical ICU of a university medical center from January 1, 2012 to June 30, 2014. Data were collected prospectively through a continuous quality improvement program on all patients intubated in the ICU over the study period. Data relating to patient demographics, intubation, and complications were analyzed. We used propensity score (propensity to use an NMBA) matching to generate 5,000 data sets of cases (failed first intubation attempts) matched to controls (successful first attempts) and conditional logistic regression to analyze the results.
Measurements and main results: There were no significant differences in patient demographics, except median total difficult airway characteristics were higher in the non-NMBA group (2 vs. 1, P < 0.001). There were significant differences in the sedative used between groups and the operator level of training. More patients who were given NMBAs received etomidate (83 vs. 35%) and more patients in the non-NMBA group received ketamine (39 vs. 9%) (P < 0.001). The FAS for NMBA use was 80.9% (401/496) compared with 69.6% (117/168) for non-NMBA use (P = 0.003). The summary odds ratio for FAS when an NMBA was used from the propensity matched analyses was 2.37 (95% confidence interval, 1.36-4.88). In the subgroup of patients intubated with a video laryngoscope, propensity-adjusted odds of FAS with the use of an NMBA was 2.50 (1.43-4.37; P < 0.001). There were no differences in procedurally related complications between groups.
Conclusions: After controlling for potential confounders, this propensity-adjusted analysis demonstrates improved odds of FAS at intubation in the ICU with the use of an NMBA. This improvement in FAS is seen even with the use of a video laryngoscope.
Keywords: airway management; intensive care; intubation; neuromuscular blockade; rapid sequence intubation.
Figures
References
-
- Mort TC. Complications of emergency tracheal intubation: hemodynamic alterations—part I. J Intensive Care Med. 2007;22:157–165. - PubMed
-
- Mort TC. Complications of emergency tracheal intubation: immediate airway-related consequences: part II. J Intensive Care Med. 2007;22:208–215. - PubMed
-
- Schwartz DE, Matthay MA, Cohen NH. Death and other complications of emergency airway management in critically ill adults: a prospective investigation of 297 tracheal intubations. Anesthesiology. 1995;82:367–376. - PubMed
-
- Reynolds SF, Heffner J. Airway management of the critically ill patient: rapid-sequence intubation. Chest. 2005;127:1397–1412. - PubMed
-
- Benedetto WJ, Hess DR, Gettings E, Bigatello LM, Toon H, Hurford WE, Schmidt U. Urgent tracheal intubation in general hospital units: an observational study. J Clin Anesth. 2007;19:20–24. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
