

Research activity and the association with mortality
- PMID: 25719608
- PMCID: PMC4342017
- DOI: 10.1371/journal.pone.0118253
Research activity and the association with mortality
Abstract
Introduction: The aims of this study were to describe the key features of acute NHS Trusts with different levels of research activity and to investigate associations between research activity and clinical outcomes.
Methods: National Institute for Health Research (NIHR) Comprehensive Clinical Research Network (CCRN) funding and number of patients recruited to NIHR Clinical Research Network (CRN) portfolio studies for each NHS Trusts were used as markers of research activity. Patient-level data for adult non-elective admissions were extracted from the English Hospital Episode Statistics (2005-10). Risk-adjusted mortality associations between Trust structures, research activity and, clinical outcomes were investigated.
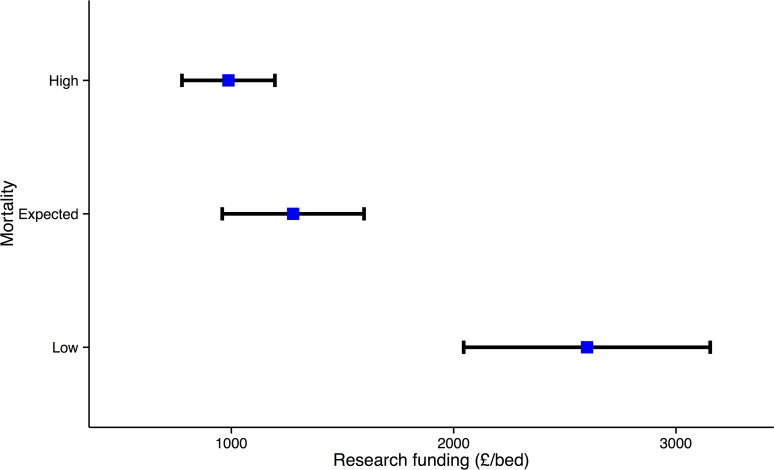
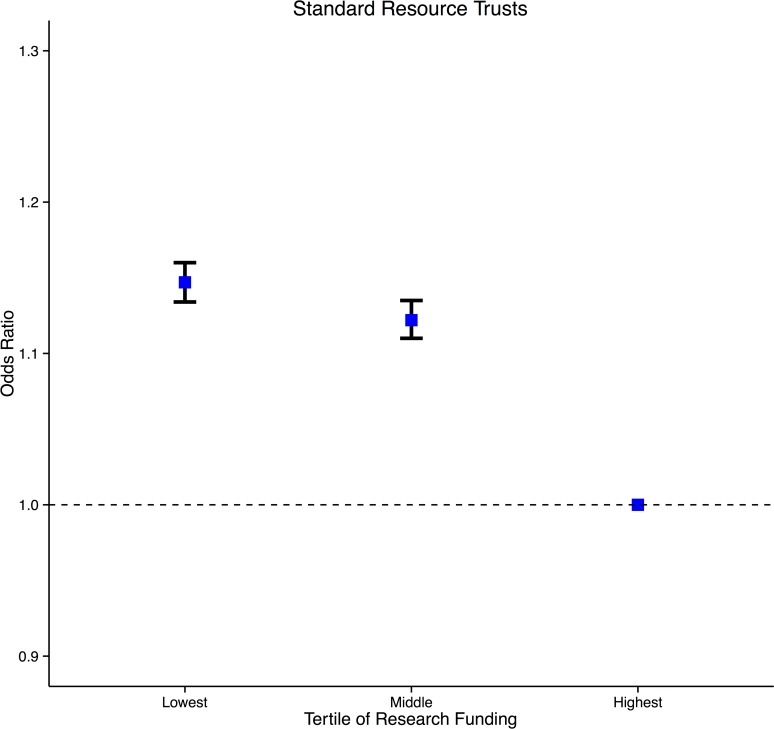
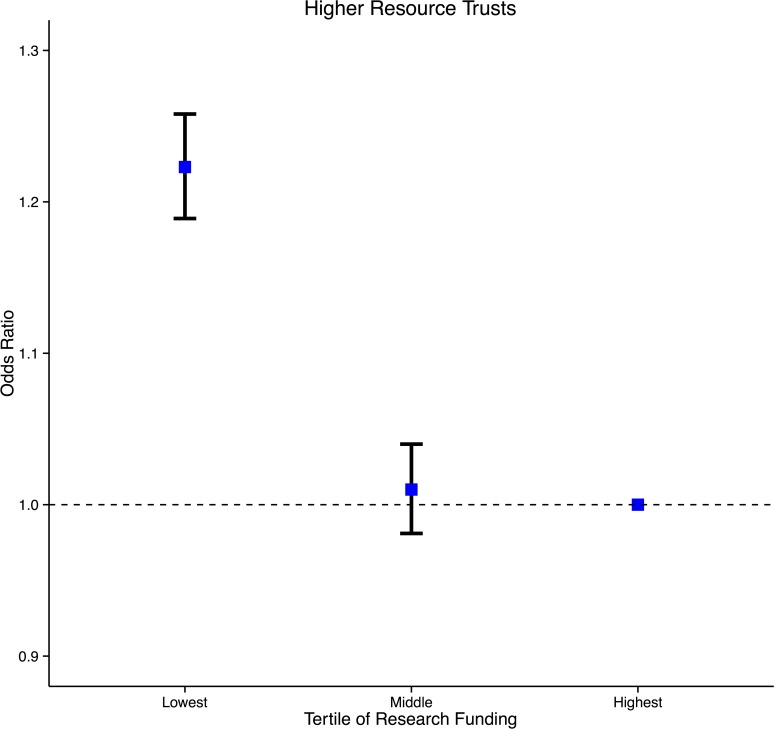
Results: Low mortality Trusts received greater levels of funding and recruited more patients adjusted for size of Trust (n = 35, 2,349 £/bed [95% CI 1,855-2,843], 5.9 patients/bed [2.7-9.0]) than Trusts with expected (n = 63, 1,110 £/bed, [864-1,357] p<0.0001, 2.6 patients/bed [1.7-3.5] p<0.0169) or, high (n = 42, 930 £/bed [683-1,177] p = 0.0001, 1.8 patients/bed [1.4-2.1] p<0.0005) mortality rates. The most research active Trusts were those with more doctors, nurses, critical care beds, operating theatres and, made greater use of radiology. Multifactorial analysis demonstrated better survival in the top funding and patient recruitment tertiles (lowest vs. highest (odds ratio & 95% CI: funding 1.050 [1.033-1.068] p<0.0001, recruitment 1.069 [1.052-1.086] p<0.0001), middle vs. highest (funding 1.040 [1.024-1.055] p<0.0001, recruitment 1.085 [1.070-1.100] p<0.0001).
Conclusions: Research active Trusts appear to have key differences in composition than less research active Trusts. Research active Trusts had lower risk-adjusted mortality for acute admissions, which persisted after adjustment for staffing and other structural factors.
Conflict of interest statement
Figures
References
-
- Research and Development Directorate. Best Research for Best Health. A new national health research strategy Department of Health; 2006. - PubMed
-
- Wright D, Milne R, Price A, Tose N. Assessing the international use of health technology assessments: exploring the merits of different methods when applied to the National Institute of Health Research Health Technology Assessment (NIHR HTA) programme. Int J Technol Assess Health Care. 2013;29: 192–197. 10.1017/S026646231300010X - DOI - PubMed
-
- Hanney S, Buxton M, Green C, Coulson D, Raferty J. An assessment of the impact of the NHS Health Technology Assessment Programme. Health Technol Assess. 2007;11: iii-iv, ix-xi, 1–180. - PubMed
-
- Hanney S, Boaz A, Jones T, Soper B. Engagement in research: an innovative three-stage review of the benefits for health-care performance. Health Serv and Deliv Res. 2013;1(8). - PubMed
-
- Druss BG, Marcus SC. Tracking publication outcomes of National Institutes of Health grants. Am J Med. 2005;118: 658–663. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
