

Secondary upper lid blepharoplasty: a clinical series using the tarsal fixation technique
- PMID: 25719715
- PMCID: PMC4342320
- DOI: 10.1097/PRS.0000000000001042
Secondary upper lid blepharoplasty: a clinical series using the tarsal fixation technique
Abstract
Background: One hundred consecutive secondary upper lid blepharoplasties were reviewed retrospectively to determine the lid characteristics of patients undergoing secondary blepharoplasty and the outcomes of all the procedures, which were performed using a tarsal fixation technique performed by one surgeon.
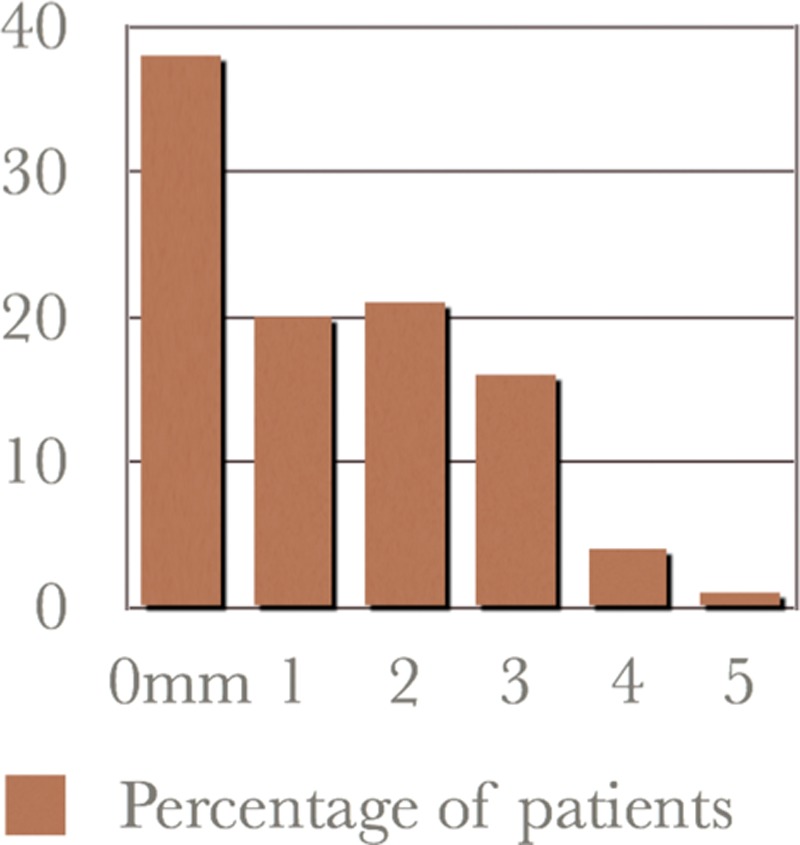
Methods: The median age of the patients was 54 years, and 99 percent of the patients were women. The median time since primary blepharoplasty was 8.7 years (range, 2 to 22 years). At surgery, no additional skin was removed in 37 percent, and the median amount excised in the remainder was only 2 mm. Revision surgery was performed in 13 percent, mainly for incomplete correction of asymmetry (5 percent) or ptosis (4 percent). Nonsurgical complications were mainly ocular (8 percent). There were no cases of persistent postoperative lagophthalmos or dry eyes.
Results: The term "postblepharoplasty look" was introduced to describe the different aging changes that follow primary blepharoplasty, mainly dermatochalasis (70 percent), with a high or absent and often poorly defined lid fold, with fat distribution irregularities. The tarsal fixation technique is advantageous in secondary blepharoplasty, as its benefit does not depend on further skin removal, minimizing the risk of lagophthalmos and dry eye syndrome. Lipoinfiltration for volume contouring is another major advance. The higher revision rate in secondary blepharoplasty reflects the incidence of asymmetry, lid ptosis, and scar from the original blepharoplasty, and from ongoing aging.
Conclusions: The postblepharoplasty look of patients undergoing secondary upper lid blepharoplasty differs from the lid appearance of patients presenting for primary blepharoplasty. Tarsal fixation and lipoinfiltration are major advances in secondary upper lid blepharoplasty.
Conflict of interest statement
Figures







References
-
- Flowers R. Optimal procedure in secondary blepharoplasty: Blepharoplasty and periorbital aesthetic surgery. Clin Plast Surg. 1993;20:225–237. - PubMed
-
- May JW, Jr, Fearon J, Zingarelli P. Retro-orbicularis oculus fat (ROOF) resection in aesthetic blepharoplasty: A 6-year study in 63 patients. Plast Reconstr Surg. 1990;86:682–689. - PubMed
-
- Flowers RS. Blepharoplasty. In: Courtiss EH, editor. In: Male Aesthetic Surgery. St. Louis: Mosby; 1982. pp. 207–239.
-
- Flowers R. Upper blepharoplasty by eyelid invagination: Anchor blepharoplasty. Clin Plast Surg. 1993;20:193–207. - PubMed
-
- Siegal R. Surgical anatomy of the upper eyelid fascia. Ann Plast Surg. 1984;13:263–273. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
