

Clinical chorioamnionitis at term I: microbiology of the amniotic cavity using cultivation and molecular techniques
- PMID: 25720095
- PMCID: PMC5881909
- DOI: 10.1515/jpm-2014-0249
Clinical chorioamnionitis at term I: microbiology of the amniotic cavity using cultivation and molecular techniques
Abstract
Introduction: The objectives of this study were: 1) to determine the amniotic fluid (AF) microbiology of patients with the diagnosis of clinical chorioamnionitis at term using both cultivation and molecular techniques; and 2) to examine the relationship between intra-amniotic inflammation with and without microorganisms and placental lesions consistent with acute AF infection.
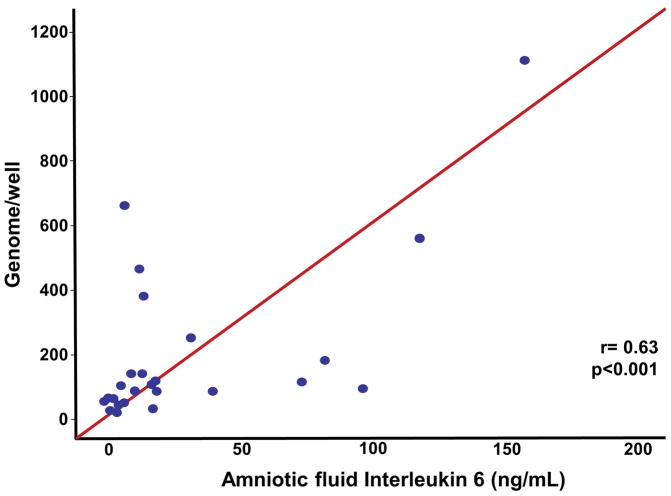
Methods: The AF samples obtained by transabdominal amniocentesis from 46 women with clinical signs of chorioamnionitis at term were analyzed using cultivation techniques (for aerobic and anerobic bacteria as well as genital mycoplasmas) and broad-range polymerase chain reaction (PCR) coupled with electrospray ionization mass spectrometry (PCR/ESI-MS). The frequency of microbial invasion of the amniotic cavity (MIAC), intra-amniotic inflammation [defined as an AF interleukin 6 (IL-6) concentration ≥2.6 ng/mL], and placental lesions consistent with acute AF infection (acute histologic chorioamnionitis and/or acute funisitis) were examined according to the results of AF cultivation and PCR/ESI-MS as well as AF IL-6 concentrations.
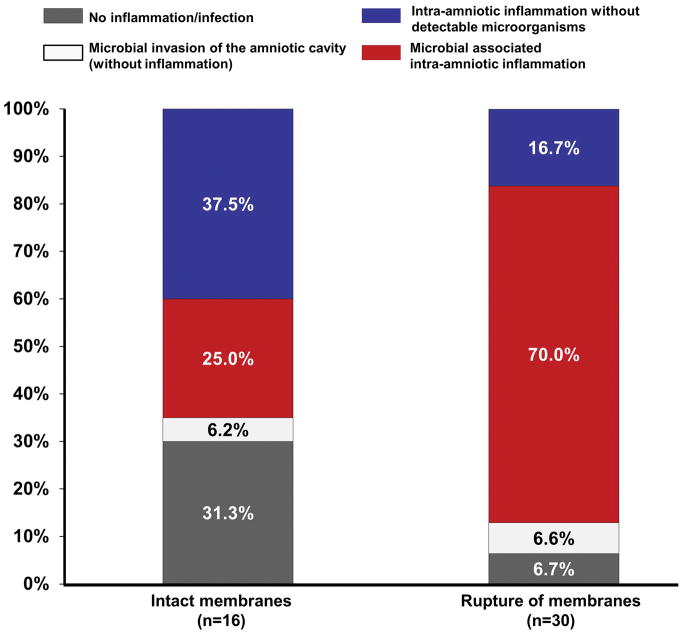
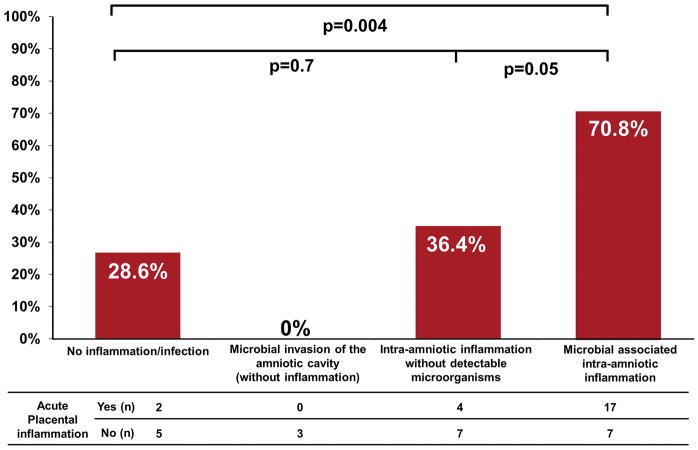
Results: 1) Culture identified bacteria in AF from 46% (21/46) of the participants, whereas PCR/ESI-MS was positive for microorganisms in 59% (27/46) – combining these two tests, microorganisms were detected in 61% (28/46) of patients with clinical chorioamnionitis at term. Eight patients had discordant test results; one had a positive culture and negative PCR/ESI-MS result, whereas seven patients had positive PCR/ESI-MS results and negative cultures. 2) Ureaplasma urealyticum (n=8) and Gardnerella vaginalis (n=10) were the microorganisms most frequently identified by cultivation and PCR/ESI-MS, respectively. 3) When combining the results of AF culture, PCR/ESI-MS and AF IL-6 concentrations, 15% (7/46) of patients did not have intra-amniotic inflammation or infection, 6.5% (3/46) had only MIAC, 54% (25/46) had microbial-associated intra-amniotic inflammation, and 24% (11/46) had intra-amniotic inflammation without detectable microorganisms. 4) Placental lesions consistent with acute AF infection were significantly more frequent in patients with microbial-associated intra-amniotic inflammation than in those without intra-amniotic inflammation [70.8% (17/24) vs. 28.6% (2/7); P=0.04].
Conclusion: Microorganisms in the AF were identified in 61% of patients with clinical chorioamnionitis at term; 54% had microbial-associated intra-amniotic inflammation, whereas 24% had intra-amniotic inflammation without detectable microorganisms.
Figures
References
-
- Malloy MH. Chorioamnionitis: epidemiology of newborn management and outcome United States 2008. J Perinatol. 2014;34:611–5. - PubMed
-
- Rouse DJ, Landon M, Leveno KJ, Leindecker S, Varner MW, Caritis SN, et al. The maternal-fetal medicine units cesarean registry: chorioamnionitis at term and its duration-relationship to outcomes. Am J Obstet Gynecol. 2004;191:211–6. - PubMed
-
- Newton ER. Chorioamnionitis and intraamniotic infection. Clin Obstet Gynecol. 1993;36:795–808. - PubMed
-
- Gibbs RS, Blanco JD, St Clair PJ, Castaneda YS. Quantitative bacteriology of AF from women with clinical intraamniotic infection at term. J Infect Dis. 1982;145:1–8. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources