

Cognitive training for attention-deficit/hyperactivity disorder: meta-analysis of clinical and neuropsychological outcomes from randomized controlled trials
- PMID: 25721181
- PMCID: PMC4382075
- DOI: 10.1016/j.jaac.2014.12.010
Cognitive training for attention-deficit/hyperactivity disorder: meta-analysis of clinical and neuropsychological outcomes from randomized controlled trials
Erratum in
- J Am Acad Child Adolesc Psychiatry. 2015 May;54(5):433
Abstract
Objective: The authors performed meta-analyses of randomized controlled trials to examine the effects of cognitive training on attention-deficit/hyperactivity disorder (ADHD) symptoms, neuropsychological deficits, and academic skills in children/adolescents with ADHD.
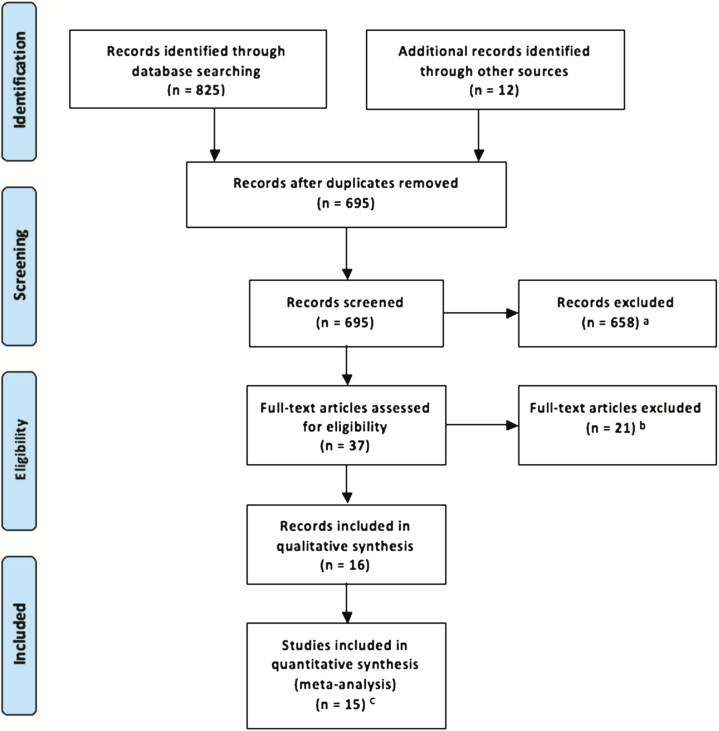
Method: The authors searched Pubmed, Ovid, Web of Science, ERIC, and CINAHAL databases through May 18, 2014. Data were aggregated using random-effects models. Studies were evaluated with the Cochrane risk of bias tool.
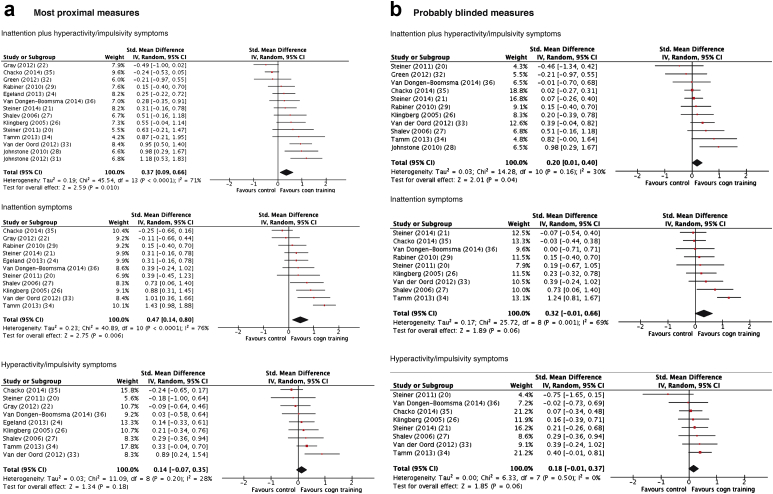
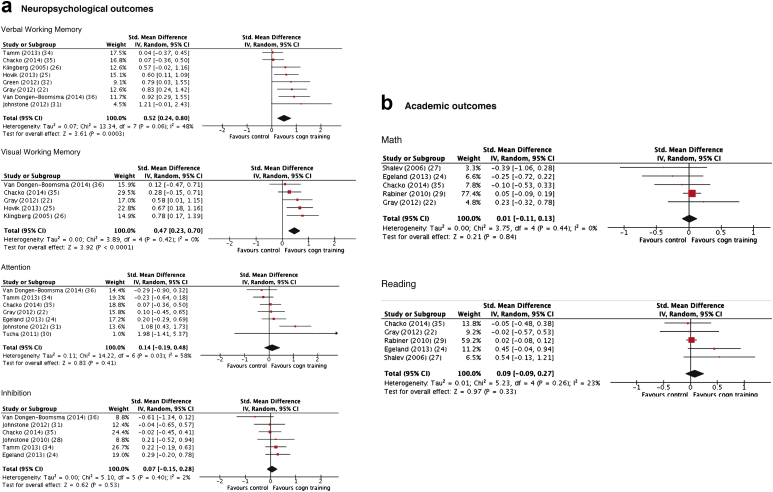
Results: Sixteen of 695 nonduplicate records were analyzed (759 children with ADHD). When all types of training were considered together, there were significant effects on total ADHD (standardized mean difference [SMD] = 0.37, 95% CI = 0.09-0.66) and inattentive symptoms (SMD = 0.47, 95% CI = 0.14-0.80) for reports by raters most proximal to the treatment setting (i.e., typically unblinded). These figures decreased substantially when the outcomes were provided by probably blinded raters (ADHD total: SMD = 0.20, 95% CI = 0.01-0.40; inattention: SMD = 0.32, 95% CI = -0.01 to 0.66). Effects on hyperactivity/impulsivity symptoms were not significant. There were significant effects on laboratory tests of working memory (verbal: SMD = 0.52, 95% CI = 0.24-0.80; visual: SMD = 0.47, 95% CI = 0.23-0.70) and parent ratings of executive function (SMD = 0.35, 95% CI = 0.08-0.61). Effects on academic performance were not statistically significant. There were no effects of working memory training, specifically on ADHD symptoms. Interventions targeting multiple neuropsychological deficits had large effects on ADHD symptoms rated by most proximal assessors (SMD = 0.79, 95% CI = 0.46-1.12).
Conclusion: Despite improving working memory performance, cognitive training had limited effects on ADHD symptoms according to assessments based on blinded measures. Approaches targeting multiple neuropsychological processes may optimize the transfer of effects from cognitive deficits to clinical symptoms.
Keywords: ADHD; evidence-based psychiatry; executive functions; nonpharmacological; working memory.
Copyright © 2015 American Academy of Child and Adolescent Psychiatry. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Ramos-Quiroga J.A., Montoya A., Kutzelnigg A., Deberdt W., Sobanski E. Attention deficit hyperactivity disorder in the European adult population: prevalence, disease awareness, and treatment guidelines. Curr Med Res Opin. 2013;29:1093–1104. - PubMed
-
- Taylor E., Dopfner M., Sergeant J. European Clinical Guidelines for Hyperkinetic Disorder—first upgrade. Eur Child Adolesc Psychiatry. 2004;13(Suppl 1):I7–I30. - PubMed
-
- Cortese S., Holtmann M., Banaschewski T. Practitioner review: current best practice in the management of adverse events during treatment with ADHD medications in children and adolescents. J Child Psychol Psychiatry. 2013;54:227–246. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
