

Child/Adolescent anxiety multimodal study: evaluating safety
- PMID: 25721183
- PMCID: PMC4362776
- DOI: 10.1016/j.jaac.2014.12.015
Child/Adolescent anxiety multimodal study: evaluating safety
Abstract
Objective: To evaluate the frequency of adverse events (AEs) across 4 treatment conditions in the Child/Adolescent Anxiety Multimodal Study (CAMS), and to compare the frequency of AEs between children and adolescents.
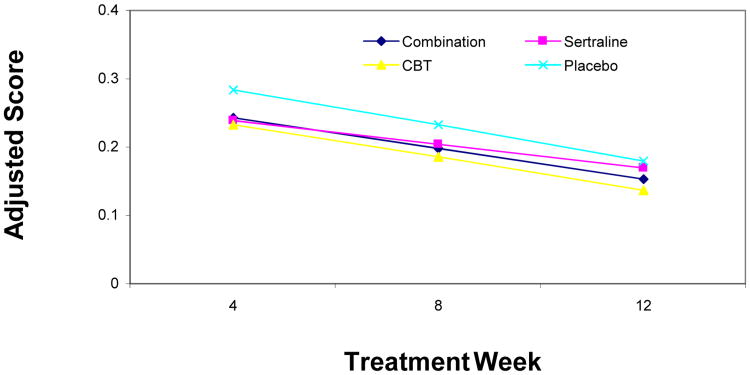
Method: Participants ages 7 to 17 years (mean = 10.7 years) meeting the DSM-IV criteria for 1 or more of the following disorders: separation anxiety disorder, generalized anxiety disorder, or social phobia were randomized (2:2:2:1) to cognitive-behavioral therapy (CBT, n = 139), sertraline (SRT, n = 133), a combination of both (COMB, n = 140), or pill placebo (PBO, n = 76). Data on AEs were collected via a standardized inquiry method plus a self-report Physical Symptom Checklist (PSC).
Results: There were no differences between the double-blinded conditions (SRT versus PBO) for total physical and psychiatric AEs or any individual physical or psychiatric AEs. The rates of total physical AEs were greater in the SRT-alone treatment condition when compared to CBT (p < .01) and COMB (p < .01). Moreover, those who received SRT alone reported higher rates of several physical AEs when compared to COMB and CBT. The rate of total psychiatric AEs was higher in children (≤12 years) across all arms (31.7% versus 23.1%, p < .05). Total PSC scores decreased over time, with no significant differences between treatment groups.
Conclusion: The results support the tolerability/safety of selective serotonin reuptake inhibitor (SSRI) treatment for anxiety disorders even after adjusting for the number of reporting opportunities, leading to no differences in overall rates of AEs. Few differences occurred on specific items. Additional monitoring of psychiatric AEs is recommended in children (≤12 years). Clinical trial registration information-Child and Adolescent Anxiety Disorders (CAMS); http://clinicaltrials.gov; NCT00052078.
Keywords: adverse events; anxiety; selective serotonin reuptake inhibitors.
Copyright © 2015 American Academy of Child and Adolescent Psychiatry. All rights reserved.
Figures
Comment in
-
Child/Adolescent Anxiety Multimodal Study safety.J Am Acad Child Adolesc Psychiatry. 2015 Mar;54(3):162-3. doi: 10.1016/j.jaac.2014.12.009. J Am Acad Child Adolesc Psychiatry. 2015. PMID: 25721180 No abstract available.
References
-
- Costello EJ, Egger HL, Angold A. The Developmental Epidemiology of Anxiety Disorders: Phenomenology, Prevalence, and Comorbidity. Child Adolesc Psychiatr Clin N Am. 2005;14(4):631–648. - PubMed
-
- Dweck CS, Wortman CB. Series in Clinical and Community Psychology: Achievement, Stress, and Anxiety. Washington, DC: Hemisphere; 1982. Learned helplessness, anxiety, and achievement motivation: Neglected parallels in cognitive, affective, and coping responses; pp. 93–125.
-
- Strauss CC, Lease CA, Kazdin AE, Dulcan MK, Last CG. Multimethod assessment of the social competence of children with anxiety disorders. J Clin Child Psychol. 1989;18(2):184–189.
-
- Kendall PC, Safford S, Flannery-Schroeder E, Webb A. Child Anxiety Treatment: Outcomes in Adolescence and Impact on Substance Use and Depression at 7.4-Year Follow-Up. J Consult Clin Psychol. 2004;72(2):276–287. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
