

Urolithiasis--an interdisciplinary diagnostic, therapeutic and secondary preventive challenge
- PMID: 25721435
- PMCID: PMC4349965
- DOI: 10.3238/arztebl.2015.0083
Urolithiasis--an interdisciplinary diagnostic, therapeutic and secondary preventive challenge
Abstract
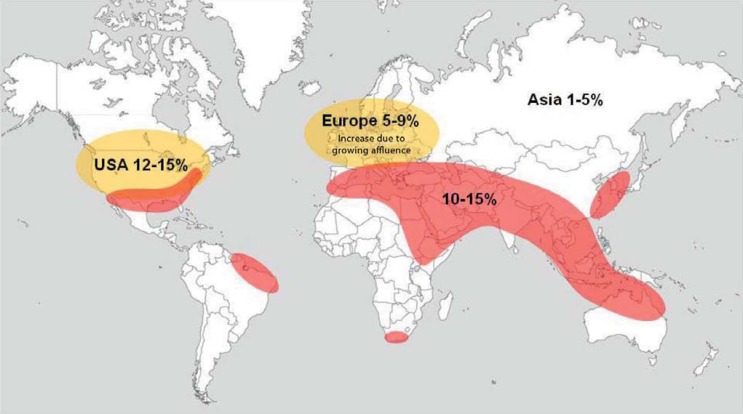
Background: The prevalence of urolithiasis in Germany is 4.7%; its incidence has trebled in the last three decades. The risk of recurrence is 50-80%, depending on the type of stone, unless secondary prevention is instituted. Risk-adapted secondary prevention lowers this risk to 10-15%.
Methods: This review is based on publications retrieved by a selective search in PubMed using the key words "urolithiasis," "urinary stones," "epidemiology," "lithogenesis," "biominerals," "risk factors," and "diagnosis, therapy, metaphylaxis." These publications were evaluated with the aid of the urolithiasis guideline of the European Association of Urology.
Results: Acute renal colic can usually be diagnosed without sophisticated equipment. Stones can be dealt with by a variety of techniques depending on their size and location, including extracorporeal shock-wave lithotripsy, ureterorenoscopy, percutaneous nephrolitholapaxy, and open surgery. Most ureteric stones of diameter up to 5 mm pass spontaneously. 75% of patients have no complications. The basic evaluation needed for secondary prevention can be carried out by any physician on an ambulatory basis. In the 25% of patients who have complications, a more extensive interdisciplinary evaluation of metabolic parameters should be performed in a clinical center for urinary stones.
Conclusion: Urolithiasis has many causes and can be treated in many different ways. An extensive metabolic work-up is often necessary for secondary prevention. The various treatment options must be considered for their suitability in each individual patient. Robust data are now available on surgical and interventional methods, but there are as yet no high-quality trials of secondary prevention. Further research should concentrate on the etiology and pathogenesis of urolithiasis.
Figures
References
-
- Koch H, Brenner G, Kerek-Bodden H. Die 50 häufigsten Diagnosestellungen (ICD-10-Schlüsselnummern) des Gesamtjahres 2006 für 12 ausgewählte Fachgebiete. Zentralinstitut für die kassenärztliche Versorgung in der Bundesrepublik Deutschland. 2007
-
- Hesse A, Bach D. Stuttgart: Thieme Verlag; 1982. Harnsteine.
-
- Bichler K, Strohmaier WL, Eipper E, Lahme S. Bichler K, editor. Epidemiologie: Das Harnsteinleiden. GEK-Edition. Lehmanns Media - LOB.de. 2007;52:31–44.
-
- Hesse A, Brandle E, Wilbert D, Kohrmann KU, Alken P. Study on the prevalence and incidence of urolithiasis in Germany comparing the years 1979 vs 2000. Eur Urol 2003. 44:709–713. - PubMed
-
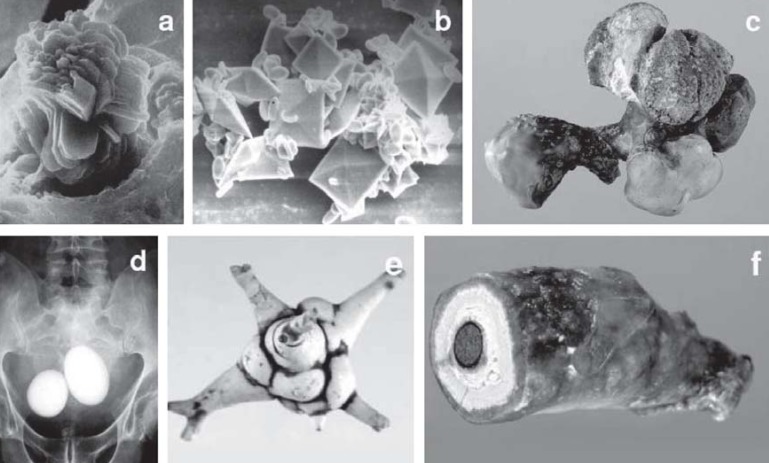
- Schubert G. Stone analysis. Urol Res. 2006;34:146–150. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources