

A case of primary adenocarcinoma of the third portion of the duodenum resected by laparoscopic and endoscopic cooperating surgery
- PMID: 25723745
- PMCID: PMC4392333
- DOI: 10.1016/j.ijscr.2015.02.031
A case of primary adenocarcinoma of the third portion of the duodenum resected by laparoscopic and endoscopic cooperating surgery
Abstract
Introduction: We report a case of primary adenocarcinoma in the third portion of the duodenum (D3) curatively resected by laparoscopic and endoscopic cooperating surgery (LECS).
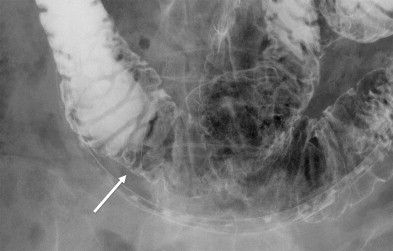
Presentation of case: A 65-year-old woman had a routine visit to our hospital for a follow-up of rectal cancer resected curatively 2 years ago. A routine screening gastroduodenal endoscopy revealed an elevated lesion of 20mm in diameter in the D3. The preoperative diagnosis was adenoma with high-grade dysplasia; however, suspicion about potential adenocarcinoma was undeniable. Curative resection was performed by LECS. Pathological examination revealed intramucosal adenocarcinoma arising from normal duodenal mucosa. The tumor was stage I (T1/N0/M0) in terms of the tumor, nodes, metastasis (TNM) classification. LECS for duodenal tumor has seldom been reported previously, and this is the first report of LECS for primary adenocarcinoma in the D3. The transverse mesocolon was removed from the head of pancreas to expose the duodenum, and the accessory right colic vein was cut; this was followed by the Kocher maneuver for mobilization of the lesion site.
Discussion: LECS enabled en bloc resection with adequate surgical margins and secure intra-abdominal suturing. Thorough mobilization of the mesocolon and pancreas head is essential for this procedure because it facilitates correct resection and suturing.
Conclusion: LECS is a feasible treatment option for duodenal neoplasms, including intramucosal adenocarcinoma, even though it exists in the D3.
Keywords: Duodenal adenocarcinoma; Duodenum; Laparoscopic and endoscopic cooperating surgery.
Copyright © 2015 The Authors. Published by Elsevier Ltd.. All rights reserved.
Figures




References
-
- Goldner B., Stabile B.E. Duodenal adenocarcinoma: why the extreme rarity of the duodenal bulb primary tumors? Am. Surg. 2014;80:956–959. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
