

Treatment of giant hiatal hernia by laparoscopic Roux-en-Y gastric bypass
- PMID: 25723747
- PMCID: PMC4392324
- DOI: 10.1016/j.ijscr.2015.02.026
Treatment of giant hiatal hernia by laparoscopic Roux-en-Y gastric bypass
Abstract
Introduction: Obesity is a risk factor for hiatal hernia. In addition, much higher recurrence rates are reported after standard surgical treatment of hiatal hernia in morbidly obese patients. Laparoscopic Roux-en-Y gastric bypass (LRYGB) is an effective surgical treatment for morbid obesity and is known to effectively control symptoms of gastroesophageal reflux (GERD).
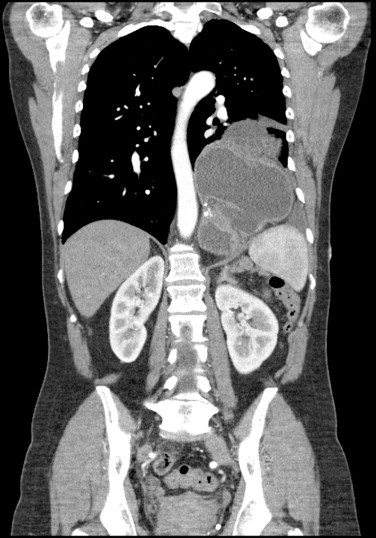
Case presentation: Two patients suffering from giant hiatal hernias where a combined LRYGB and hiatal hernia repair (HHR) with mesh was performed are presented in this paper. There were no postoperative complications and at 1 year follow-up, there was no sign of recurrence of the hernia.
Discussion: The gold standard for all symptomatic reflux patients is still surgical correction of the paraesophageal hernia, including complete reduction of the hernia sac, resection of the sac, hiatal closure and fundoplication. However, HHR outcome is adversely affected by higher BMI levels, leading to increased HH recurrence rates in the obese.
Conclusion: Concomitant giant hiatal hernia repair with LRYGB appears to be safe and feasible. Moreover, LRYGB plus HHR appears to be a good alternative for HH patients suffering from morbid obesity as well than antireflux surgery alone because of the additional benefit of significant weight loss and improvement of obesity related co-morbidity.
Keywords: Bariatric; GERD; Hiatal paraesophageal hernia; Laparoscopic gastric bypass; Morbid obesity; Surgery.
Copyright © 2015 The Authors. Published by Elsevier Ltd.. All rights reserved.
Figures
References
-
- Nocon M., Labenz J., Willich S.N. Lifestyle factors and symptoms of gastro-oesophageal reflux – a population-based study. Aliment. Pharmacol. Ther. 2006;23:169–174. - PubMed
-
- Hampel H., Abraham N.S., El-Serag H.B. Meta-analysis: obesity and the risk for gastroesophageal reflux disease and its complications. Ann. Intern. Med. 2005;143:199–211. - PubMed
-
- Perez A.R., Moncure A.C., Rattner D.W. Obesity adversely affects the outcome of antireflux operations. Surg. Endosc. 2001;15:986–996. - PubMed
-
- Salvador-Sanchis J.L., Martinez-Ramos D., Herfarth A., Rivadulla-Serrano I., Ibanez-Belenguer M., Hoashi J.S. Treatment of morbid obesity and hiatal paraesophageal hernia by laparoscopic Roux-en-Y gastric bypass. Obes. Surg. 2010;20:801–803. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
