

An Evaluation of Cerebral and Systemic Predictors of 18-Month Outcomes for Neonates With Hypoxic Ischemic Encephalopathy
- PMID: 25724376
- PMCID: PMC4551612
- DOI: 10.1177/0883073815573319
An Evaluation of Cerebral and Systemic Predictors of 18-Month Outcomes for Neonates With Hypoxic Ischemic Encephalopathy
Abstract
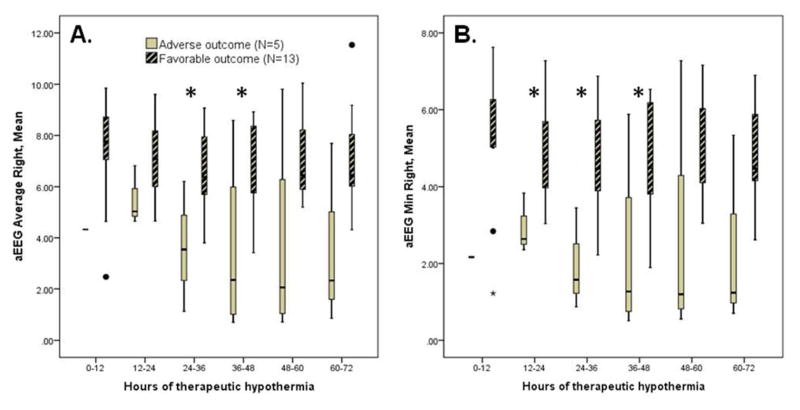
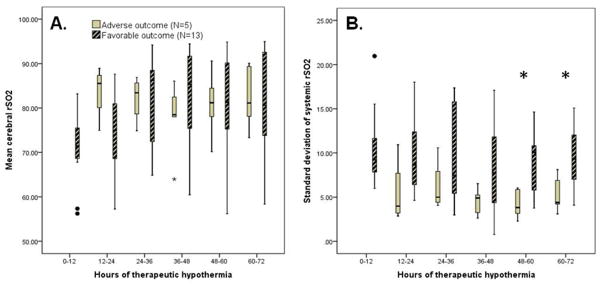
Amplitude-integrated EEG (aEEG) is a commonly used predictor of outcome after hypoxic ischemic encephalopathy. Cerebral and systemic near-infrared spectroscopy and acute kidney injury might also have prognostic value. The authors monitored neonates with aEEG, cerebral and systemic near-infrared spectroscopy during therapeutic hypothermia, assigned an acute kidney injury stage, and measured neurodevelopmental outcome. For 18 infants, cerebral near-infrared spectroscopy variables did not differentiate between those with favorable (n = 13) versus adverse (death or moderate-severe disability; n = 5) 18-month outcomes. However, systemic rSO2 variability was higher during hours 48-72 of cooling among those with favorable outcomes (.02 < P < .03). Mean aEEG amplitude during hours 24 to 48 of cooling was higher among those with good outcomes (.027 < P < .032). The aEEG lower margin was also higher during hours 12 to 48 for those with good outcomes (.014 < P < .035). Acute kidney injury did not predict outcome (P > .05). aEEG is a useful prognostic tool for outcomes after neonatal hypoxic ischemic encephalopathy, but the role of near-infrared spectroscopy in the hypothermia-treated population remains uncertain.
Keywords: acute kidney injury; amplitude-integrated EEG; developmental outcome; hypoxic-ischemic encephalopathy; near-infrared spectroscopy.
© The Author(s) 2015.
Conflict of interest statement
Declaration of Conflicts of Interest:
Dr. Shellhaas receives research funding from NIH, the Child Neurology Foundation, and intramural grants from the University of Michigan’s Department of Pediatrics and Communicable Diseases. She serves on the editorial boards of
J. Kushwaha and M. Plegue have nothing to disclose.
D. Selewski receives research funding from the Renal Research Institute and intramural grants from the University of Michigan’s Department of Pediatrics and Communicable Diseases.
J. Barks receives research funding from NIH.
Figures
References
-
- Azzopardi DV, Strohm B, Edwards AD, et al. Moderate hypothermia to treat perinatal asphyxial encephalopathy. New England Journal of Medicine. 2009;361:1349–58. - PubMed
-
- Shankaran S, Laptook AR, Ehrenkranz RA, et al. Whole body hypothermia for neonates with hypoxic-ischemic encephalopathy. New England Journal of Medicine. 2005;353:1574–84. - PubMed
-
- Gluckman PD, Wyatt JS, Azzopardi D, et al. Selective head cooling with mild systemic hypothermia after neonatal encephalopathy: multicentre randomised trial. Lancet. 2005;365:663–70. - PubMed
-
- Guillet R, Edwards AD, Thoresen M, et al. Seven- to eight-year follow-up of the CoolCap trial of head cooling for neonatal encephalopathy. Pediatric Research. 2012;71:205–9. - PubMed
-
- Azzopardi D, Strohm B, Marlow N, et al. Effects of hypothermia for perinatal asphyxia on childhood outcomes. New England Journal of Medicine. 2014;371:140–9. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
