

Automated, electronic alerts for acute kidney injury: a single-blind, parallel-group, randomised controlled trial
- PMID: 25726515
- PMCID: PMC4475457
- DOI: 10.1016/S0140-6736(15)60266-5
Automated, electronic alerts for acute kidney injury: a single-blind, parallel-group, randomised controlled trial
Abstract
Background: Acute kidney injury often goes unrecognised in its early stages when effective treatment options might be available. We aimed to determine whether an automated electronic alert for acute kidney injury would reduce the severity of such injury and improve clinical outcomes in patients in hospital.
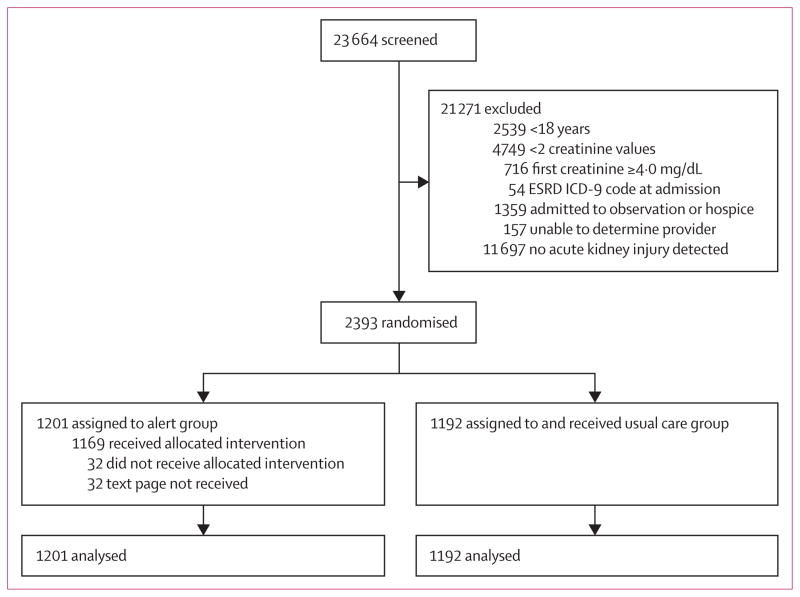
Methods: In this investigator-masked, parallel-group, randomised controlled trial, patients were recruited from the hospital of the University of Pennsylvania in Philadelphia, PA, USA. Eligible participants were adults aged 18 years or older who were in hospital with stage 1 or greater acute kidney injury as defined by Kidney Disease Improving Global Outcomes creatinine-based criteria. Exclusion criteria were initial hospital creatinine 4·0 mg/dL (to convert to μmol/L, multiply by 88·4) or greater, fewer than two creatinine values measured, inability to determine the covering provider, admission to hospice or the observation unit, previous randomisation, or end-stage renal disease. Patients were randomly assigned (1:1) via a computer-generated sequence to receive an acute kidney injury alert (a text-based alert sent to the covering provider and unit pharmacist indicating new acute kidney injury) or usual care, stratified by medical versus surgical admission and intensive care unit versus non-intensive care unit location in blocks of 4-8 participants. The primary outcome was a composite of relative maximum change in creatinine, dialysis, and death at 7 days after randomisation. All analyses were by intention to treat. This study is registered with ClinicalTrials.gov, number NCT01862419.
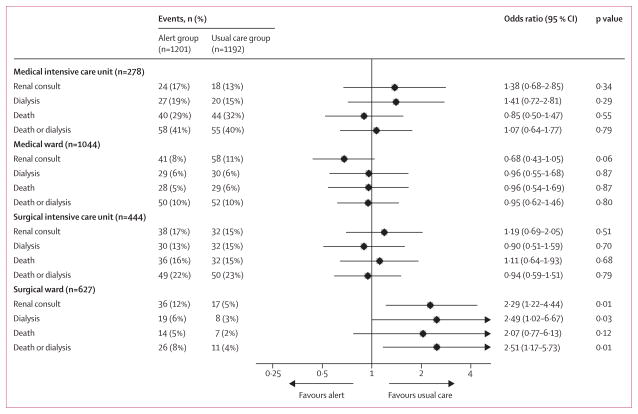
Findings: Between Sept 17, 2013, and April 14, 2014, 23,664 patients were screened. 1201 eligible participants were assigned to the acute kidney injury alert group and 1192 were assigned to the usual care group. Composite relative maximum change in creatinine, dialysis, and death at 7 days did not differ between the alert group and the usual care group (p=0·88), or within any of the four randomisation strata (all p>0·05). At 7 days after randomisation, median maximum relative change in creatinine concentrations was 0·0% (IQR 0·0-18·4) in the alert group and 0·6% (0·0-17·5) in the usual care group (p=0·81); 87 (7·2%) patients in the alert group and 70 (5·9%) patients in usual care group had received dialysis (odds ratio 1·25 [95% CI 0·90-1·74]; p=0·18); and 71 (5·9%) patients in the alert group and 61 (5·1%) patients in the usual care group had died (1·16 [0·81-1·68]; p=0·40).
Interpretation: An electronic alert system for acute kidney injury did not improve clinical outcomes among patients in hospital.
Funding: Penn Center for Healthcare Improvement and Patient Safety.
Copyright © 2015 Elsevier Ltd. All rights reserved.
Conflict of interest statement
FPW has a patent “A method and system for detecting and categorising disease” pending. MS reports a K23 Mentored Career Development Award from the National Institute of Health during the conduct of the study. HIF reports honorarium from Kyowa Kirin and GlaxoSmithKline outside of the submitted work. Other authors declare no competing interests.
Figures
Comment in
-
On the alert for outcome improvement in acute kidney injury.Lancet. 2015 May 16;385(9981):1924-6. doi: 10.1016/S0140-6736(15)60181-7. Epub 2015 Feb 26. Lancet. 2015. PMID: 25726516 No abstract available.
-
Acute kidney injury: Do electronic alerts for AKI improve outcomes?Nat Rev Nephrol. 2015 Jun;11(6):322-3. doi: 10.1038/nrneph.2015.55. Epub 2015 Apr 21. Nat Rev Nephrol. 2015. PMID: 25898356 No abstract available.
-
ACP Journal Club. In hospitalized patients, an electronic alert for acute kidney injury did not differ from usual care.Ann Intern Med. 2015 Jun 16;162(12):JC6. doi: 10.7326/ACPJC-2015-162-12-006. Ann Intern Med. 2015. PMID: 26075783 No abstract available.
References
-
- Andrikos E, Tseke P, Balafa O, et al. Epidemiology of acute renal failure in ICUs: a multi-center prospective study. Blood Purif. 2009;28:239–44. - PubMed
-
- Bagshaw SM, George C, Dinu I, Bellomo R. A multi-centre evaluation of the RIFLE criteria for early acute kidney injury in critically ill patients. Nephrol Dial Transplant. 2008;23:1203–10. - PubMed
-
- Bagshaw SM, Uchino S, Bellomo R, et al. Septic acute kidney injury in critically ill patients: clinical characteristics and outcomes. Clin J Am Soc Nephrol. 2007;2:431–39. - PubMed
-
- Joannidis M, Metnitz B, Bauer P, et al. Acute kidney injury in critically ill patients classified by AKIN versus RIFLE using the SAPS 3 database. Intensive Care Med. 2009;35:1692–702. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
