

Investigational agents for treatment of traumatic brain injury
- PMID: 25727893
- PMCID: PMC4433440
- DOI: 10.1517/13543784.2015.1021919
Investigational agents for treatment of traumatic brain injury
Abstract
Introduction: Traumatic brain injury (TBI) is a major cause of death and disability worldwide. To date, there are no pharmacologic agents proven to improve outcomes from TBI because all the Phase III clinical trials in TBI have failed. Thus, there is a compelling need to develop treatments for TBI.
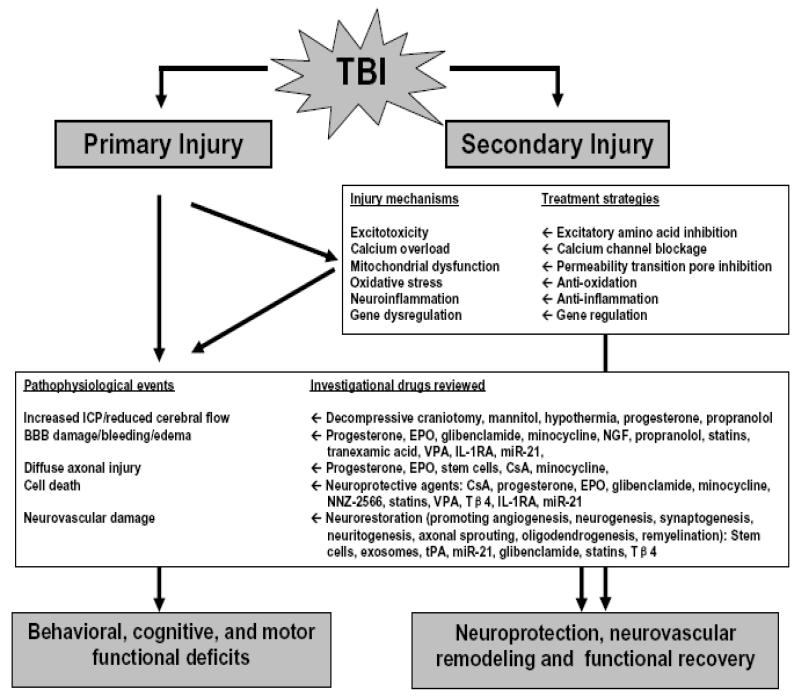
Areas covered: The following article provides an overview of select cell-based and pharmacological therapies under early development for the treatment of TBI. These therapies seek to enhance cognitive and neurological functional recovery through neuroprotective and neurorestorative strategies.
Expert opinion: TBI elicits both complex degenerative and regenerative tissue responses in the brain. TBI can lead to cognitive, behavioral, and motor deficits. Although numerous promising neuroprotective treatment options have emerged from preclinical studies that mainly target the lesion, translation of preclinical effective neuroprotective drugs to clinical trials has proven challenging. Accumulating evidence indicates that the mammalian brain has a significant, albeit limited, capacity for both structural and functional plasticity, as well as regeneration essential for spontaneous functional recovery after injury. A new therapeutic approach is to stimulate neurovascular remodeling by enhancing angiogenesis, neurogenesis, oligodendrogenesis, and axonal sprouting, which in concert, may improve neurological functional recovery after TBI.
Keywords: angiogenesis; cell therapy; exosomes; microRNAs; neurogenesis; neuroprotection; neurorestoration; traumatic brain injury.
Figures
References
-
- Menon DK, Schwab K, Wright DW, et al. Position statement: definition of traumatic brain injury. Arch Phys Med Rehabil. 2010;91(11):1637–40. - PubMed
-
- Chauhan NB. Chronic neurodegenerative consequences of traumatic brain injury. Restor Neurol Neurosci. 2014 - PubMed
-
- Hyder AA, Wunderlich CA, Puvanachandra P, et al. The impact of traumatic brain injuries: a global perspective. NeuroRehabilitation. 2007;22(5):341–53. - PubMed
-
- Langlois JA, Rutland-Brown W, Wald MM. The epidemiology and impact of traumatic brain injury: a brief overview. J Head Trauma Rehabil. 2006;21(5):375–8. - PubMed
-
- Masel BE, DeWitt DS. Traumatic brain injury: a disease process, not an event. J Neurotrauma. 2010;27(8):1529–40. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources