

Implications of the new American College of Cardiology/American Heart Association cholesterol guidelines for primary atherosclerotic cardiovascular disease event prevention in a multi ethnic cohort: Multi-Ethnic Study of Atherosclerosis (MESA)
- PMID: 25728729
- PMCID: PMC4347939
- DOI: 10.1016/j.ahj.2014.12.018
Implications of the new American College of Cardiology/American Heart Association cholesterol guidelines for primary atherosclerotic cardiovascular disease event prevention in a multi ethnic cohort: Multi-Ethnic Study of Atherosclerosis (MESA)
Abstract
Background: The impact of replacing the National Cholesterol Education Program (NCEP)/Adult Treatment Program (ATP) III cholesterol guidelines with the new 2013 American College of Cardiology (ACC)/American Heart Association (AHA) guidelines for primary prevention of cardiovascular disease is unclear.
Methods: We used risk factor and 10-year clinical event rate data from MESA, combined with estimates of efficacy of moderate and high-intensity statin therapy from meta-analyses of statin primary prevention trials to estimate (a) the change in number of subjects eligible for drug therapy and (2) the anticipated reduction in atherosclerotic cardiovascular disease (ASCVD) events and increment in type 2 diabetes mellitus (T2DM) associated with the change in cholesterol guidelines.
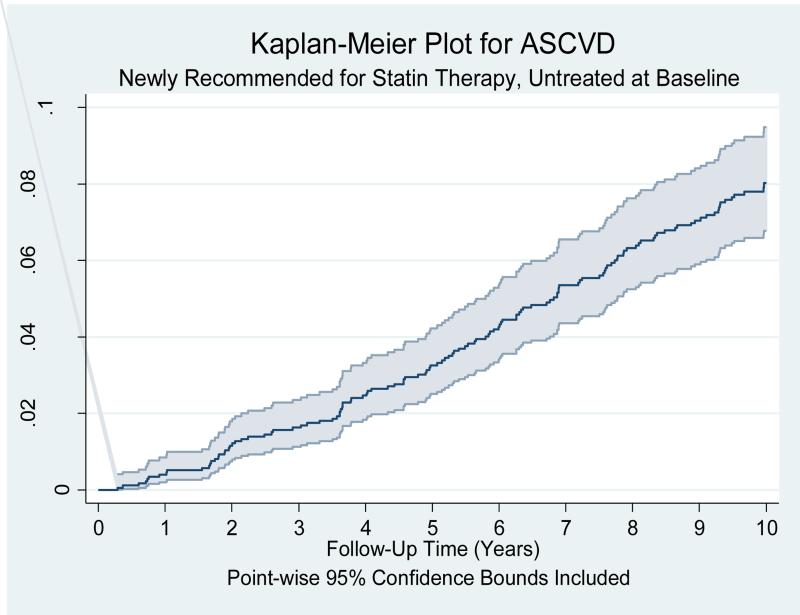
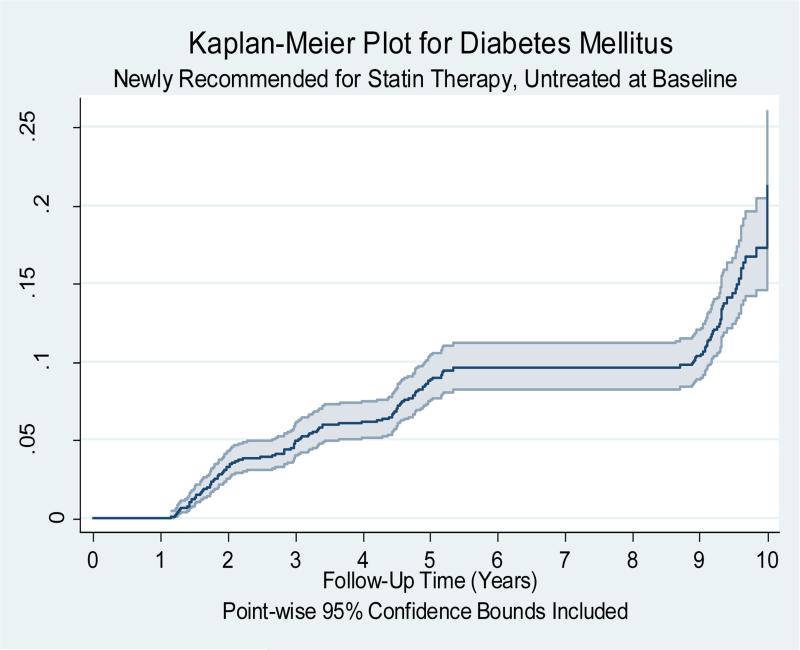
Results: Of the 6,814 MESA participants, 5,437 were not on statins at baseline and had complete data for analysis (mean age 61.4±10.3). Using the NCEP/ATP III guidelines, 1,334 (24.5%) would have been eligible for statin therapy compared with 3,015 (55.5%) under the new ACC/AHA guidelines. Among the subset of newly eligible, 127/1,742 (7.3%) had an ASCVD event during 10years of follow-up. Assuming 10years of moderate-intensity statin therapy, the estimated absolute reduction in ASCVD events for the newly eligible group was 2.06% (number needed to treat [NNT] 48.6) and the estimated absolute increase in T2DM was 0.90% (number needed to harm [NNH] 110.7). Assuming 10years of high-intensity statin therapy, the corresponding estimates for reductions in ASCVD and increases in T2DM were as follows: ASCVD 2.70% (NNT 37.5) and T2DM 2.60% (NNH 38.6). The estimated effects of moderate-intensity statins on 10-year risk for ASCVD and T2DM in participants eligible for statins under the NCEP/ATP III were as follows: 3.20% (NNT 31.5) and 1.06% (NNH 94.2), respectively.
Conclusion: Substituting the NCEP/ATP III cholesterol guidelines with the 2013 ACC/AHA cholesterol guidelines in MESA more than doubled the number of participants eligible for statin therapy. If the new ACC/AHA cholesterol guidelines are adopted and extend the primary prevention population eligible for treatment, the risk-benefit profile is much better for moderate-intensity than high-intensity statin treatment.
Copyright © 2015 Elsevier Inc. All rights reserved.
Figures
References
-
- National Cholesterol Education Program Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults, Executive summary of the third report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). JAMA. 2001;285:2486–2497. - PubMed
-
- Grundy SM, Cleeman JI, Merz CN, Brewer HB, Jr, Clark LT, Hunninghake DB, Pasternak RC, Smith SC, Jr, Stone JJ. National Heart, Lung and Blood Institute; American College of Cardiology Foundation; American Heart Association. Circulation. 2004;110:227–39. - PubMed
-
- Stone NJ, Robinson J, Lichtenstein AH, Merz CN, Blum CB, Eckel RH, Goldberg AC, Gordon D, Levy D, Lloyd-Jones DM, McBride P, Schwartz JS, Shero ST, Smith SC, Jr, Watson K, Wilson PW. ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 20132013:S0735–1097(13)06028-2. - PubMed
-
- Lenzer J. Majority of panelists on controversial new cholesterol guideline have current or recent ties to drug manufacturers. BMJ. 347(2013):f6989. - PubMed
-
- Ridker PM, Cook NR. Statins: new American guidelines for prevention of cardiovascular disease. Lancet. 2013;382:1762– 1765. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- N01-HC-95162/HC/NHLBI NIH HHS/United States
- N01 HC095161/HL/NHLBI NIH HHS/United States
- N01 HC095168/HL/NHLBI NIH HHS/United States
- N01 HC095169/HL/NHLBI NIH HHS/United States
- N01-HC-95165/HC/NHLBI NIH HHS/United States
- N01 HC095159/HL/NHLBI NIH HHS/United States
- R01HL098445/HL/NHLBI NIH HHS/United States
- UL1-TR-000040/TR/NCATS NIH HHS/United States
- N01-HC-95160/HC/NHLBI NIH HHS/United States
- N01 HC095163/HL/NHLBI NIH HHS/United States
- N01 HC095166/HL/NHLBI NIH HHS/United States
- UL1 RR025005/RR/NCRR NIH HHS/United States
- UL1-RR-025005/RR/NCRR NIH HHS/United States
- N01-HC-95163/HC/NHLBI NIH HHS/United States
- N01-HC-95168/HC/NHLBI NIH HHS/United States
- N01-HC-95159/HC/NHLBI NIH HHS/United States
- N01 HC095167/HL/NHLBI NIH HHS/United States
- N01-HC-95169/HC/NHLBI NIH HHS/United States
- N01-HC-95164/HC/NHLBI NIH HHS/United States
- R01 HL098445/HL/NHLBI NIH HHS/United States
- N01 HC095165/HC/NHLBI NIH HHS/United States
- N01-HC-95161/HC/NHLBI NIH HHS/United States
- UL1 TR000040/TR/NCATS NIH HHS/United States
- N01 HC095162/HL/NHLBI NIH HHS/United States
- N01-HC-95166/HC/NHLBI NIH HHS/United States
- N01 HC095165/HL/NHLBI NIH HHS/United States
- N01 HC095164/HL/NHLBI NIH HHS/United States
- N01-HC-95167/HC/NHLBI NIH HHS/United States
- N01 HC095160/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
