

Erectile dysfunction as a marker for cardiovascular disease diagnosis and intervention: a cost analysis
- PMID: 25728904
- PMCID: PMC4390459
- DOI: 10.1111/jsm.12848
Erectile dysfunction as a marker for cardiovascular disease diagnosis and intervention: a cost analysis
Abstract
Introduction: Erectile dysfunction (ED) is a risk factor for cardiovascular disease (CVD). We examine the costs of screening men with ED for CVD risk factors and the cost savings of treating these at risk men.
Aim: This study aims to evaluate the effect of screening men presenting with ED for CVD risk factors and to determine the cost effectiveness of this screening protocol.
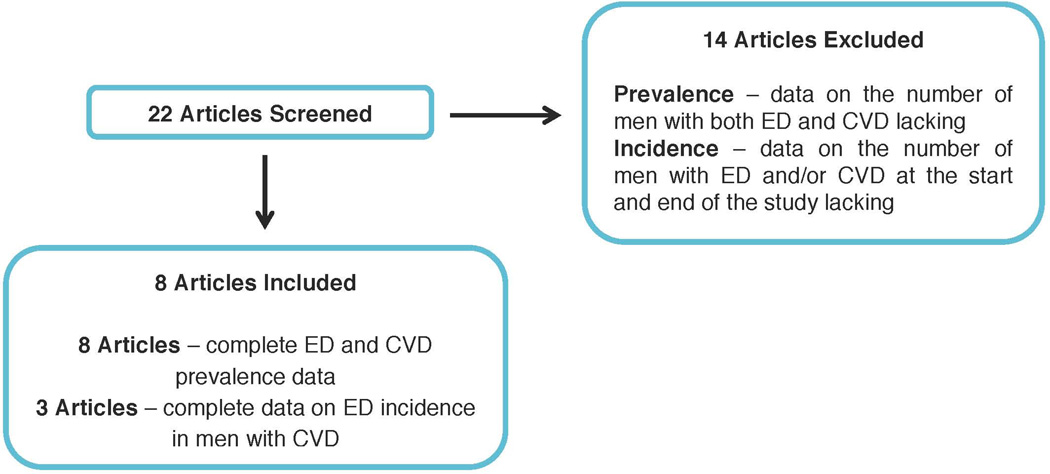
Methods: The known incidence and prevalence of ED and CVD, the rate of undiagnosed CVD, and the effects of CVD treatment were used to model the change in prevalence of acute CVD events and ED as a function of the number of men with ED and CVD. The cost savings associated with reduction in acute cardiovascular (CV) events and ED prevalence was estimated over 20 years.
Main outcome measures: Acute CVD event rate reduction and associated cost savings were modeled over 20 years.
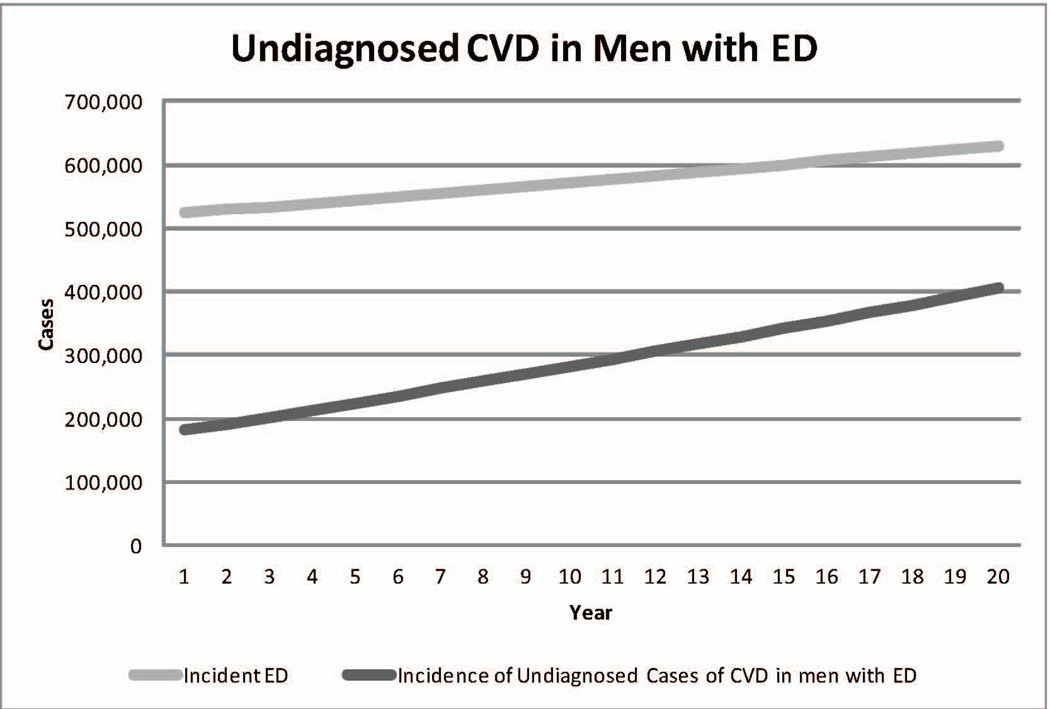
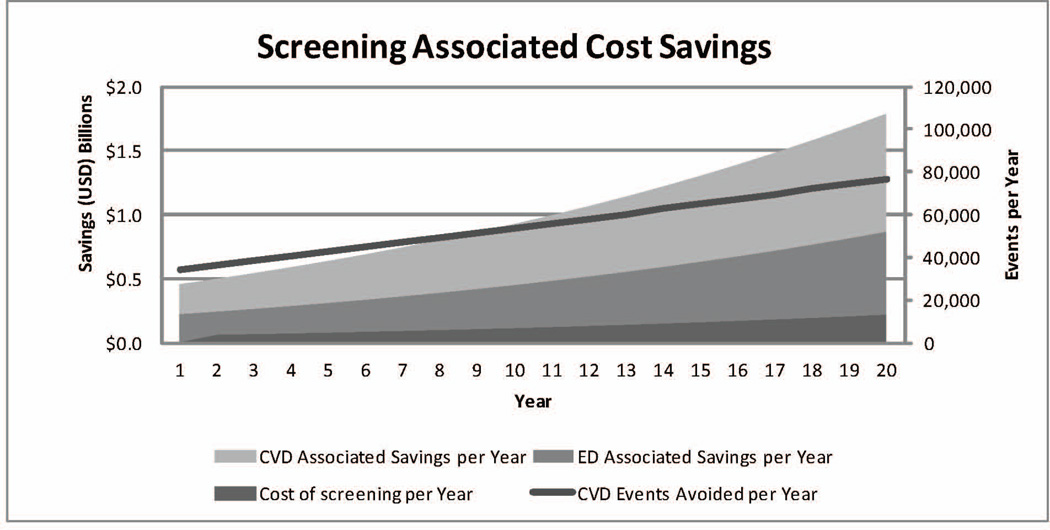
Results: The relative risk of ED in men with CVD is 1.47 and the coprevalence of both ED and CVD was estimated at 1,991,520 men. Approximately 44% of men with CVD risk factors are unaware of their risk. If all men presenting with ED were screened for CVD, 5.8 million men with previously unknown CVD risk factors would be identified over 20 years, costing $2.7 billion to screen. Assuming a 20% decrease in CV events as a result of screening and treatment, 1.1 million cardiovascular events would be avoided, saving $21.3 billion over 20 years. Similarly, 1.1 million cases of ED would be treated, saving $9.7 billion. Together, the reduction in acute CVD and ED treatment cost would save $28.5 billion over 20 years.
Conclusions: Screening for CVD in men presenting with ED can be a cost-effective intervention for secondary prevention of both CVD and, over the longer term, ED.
Keywords: Cardiovascular Disease; Cardiovascular Disease Treatment; Cardiovascular Risk Factors; Cost Analysis; Erectile Dysfunction; Erectile Dysfunction Treatment.
© 2015 International Society for Sexual Medicine.
Figures
References
-
- Saigal CS, et al. Predictors and prevalence of erectile dysfunction in a racially diverse population. Arch. Intern. Med. 2006;166:207–212. - PubMed
-
- Polinski JM, Kesselheim AS. Where Cost, Medical Necessity, and Morality Meet: Should US Government Insurance Programs Pay for Erectile Dysfunction Drugs? Clin Pharmacol Ther. 2011;89:17–19. - PubMed
-
- Gandaglia G, et al. A systematic review of the association between erectile dysfunction and cardiovascular disease. Eur. Urol. 2014;65:968–978. - PubMed
-
- Thompson IM, et al. ERectile dysfunction and subsequent cardiovascular disease. JAMA. 2005;294:2996–3002. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
