

Review
doi: 10.1152/physiol.00035.2014.
The baroreflex as a long-term controller of arterial pressure
Affiliations
- PMID: 25729060
- PMCID: PMC4346703
- DOI: 10.1152/physiol.00035.2014
Item in Clipboard
Review
The baroreflex as a long-term controller of arterial pressure
Physiology (Bethesda).
2015 Mar.
Abstract
Because of resetting, a role for baroreflexes in long-term control of arterial pressure has been commonly dismissed in the past. However, in recent years, this perspective has changed. Novel approaches for determining chronic neurohormonal and cardiovascular responses to natural variations in baroreceptor activity and to electrical stimulation of the carotid baroreflex indicate incomplete resetting and sustained responses that lead to long-term alterations in sympathetic activity and arterial pressure.
©2015 Int. Union Physiol. Sci./Am. Physiol. Soc.
Figures
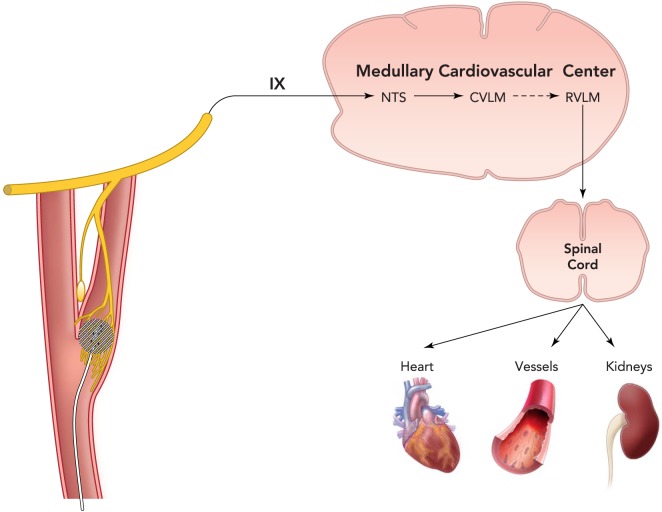
A schematic representation of the sympathetic carotid baroreflex arc including key medullary brain regions for cardiovascular control Pressure-induced stretch of carotid sinus baroreceptors is transduced into an electrical signal in afferent fibers in the carotid sinus nerve (Hering's nerve), a branch of the glossopharyngeal nerve (cranial nerve IX), and impulses then travel to the NTS, the initial central site of termination of baroreceptor afferents. In turn, NTS neurons activate inhibitory neurons in the CVLM that project to the RVLM. Projections from RVLM neurons to preganglionic neurons in the intermediolateral cell column of the spinal cord account for basal sympathetic outflow to the periphery. Thus pressure-induced baroreceptor activation of the NTS and CVLM neurons suppresses central sympathetic outflow by inhibiting the RVLM. This medullary brain circuit is also activated by electrical stimulation of the carotid sinus leading to substantial long-term reductions in sympathetic activity and arterial pressure. With the current Barostem neo system, a miniaturized stimulating electrode is sutured to the surface of the carotid sinus and is connected to an internally implantable pulse generator that is externally programmable by radiofrequency control. NTS, nucleus tractus solitarius; CVLM, caudal ventolateral medulla; RVLM, rostral ventrolateral medulla.
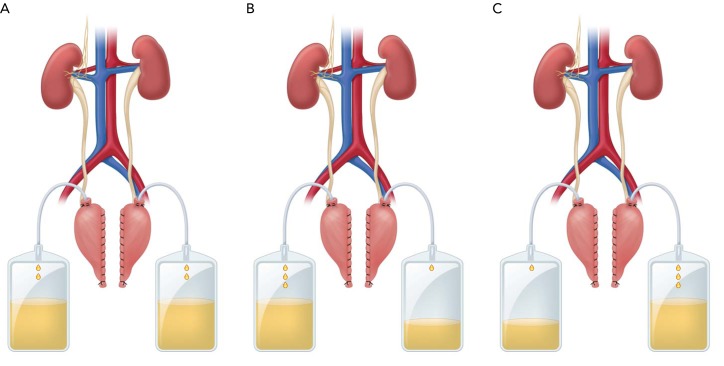
Daily sodium/fluid excretion from innervated and denervated kidneys Daily sodium/fluid excretion from innervated and denervated kidneys under control conditions (A), during ANG II hypertension (B), and during ANG II hypertension (C) after sinoaortic denervation (SAD). Sodium intake was constant, and daily sodium balance was achieved under all conditions. During ANG II hypertension, there was a relatively greater rate of sodium excretion from innervated than denervated kidneys before but not after SAD, consistent with sustained baroreflex-mediated inhibition of renal sympathetic nerve activity. In the absence of the baroreflex (C), the lower rate of sodium excretion from innervated vs. denervated kidneys may reflect central actions of ANG II to increase renal sympathetic nerve activity.
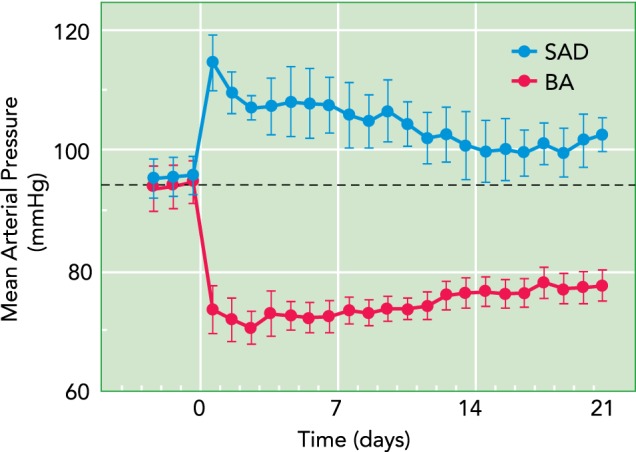
Chronic changes in mean arterial pressure following sinoaortic SAD and electrical baroreflex activation Substantial reductions in mean arterial pressure were sustained during baroreflex activation (BA), whereas increases in mean arterial pressure were transient following SAD, as expected.
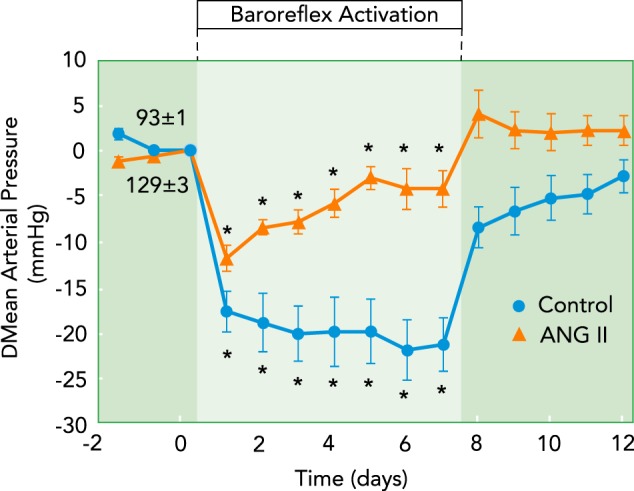
Chronic changes in mean arterial pressure during prolonged BA before and after induction of hypertension by chronic infusion of ANG II Acute reductions in arterial pressure (not shown) in response to BA were substantial and equivalent under both conditions. In contrast, whereas robust pressure reductions were sustained during BA under control conditions, they were markedly reduced in ANG II hypertension.
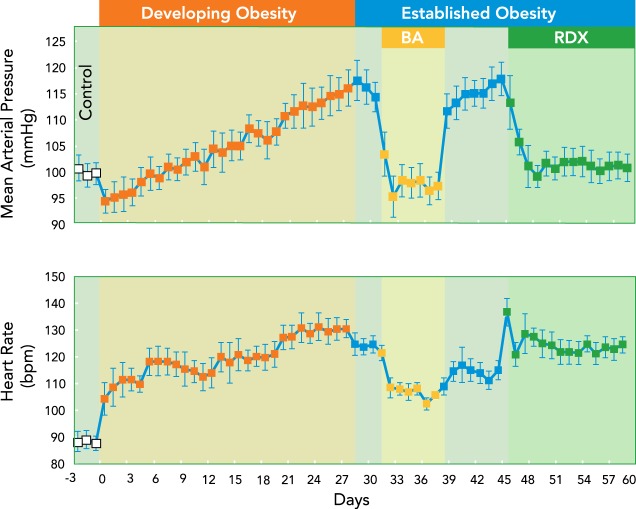
Development of hypertension with weight gain and the effects of global and renal specific sympathetic inhibition by BA and surgical renal denervation Development of hypertension with weight gain and the effects of global and renal-specific sympathetic inhibition by BA and surgical renal denervation (RDX), respectively, in the established phase of obesity. Abolition of the hypertension by RDX alone emphasizes the critical importance of increased renal sympathetic nerve activity in the pathogenesis of obesity hypertension and the critical role of renal-specific suppression of sympathetic activity in mediating the anti-hypertensive effects of BA.
References
-
- Alnima T, de Leeuw PW, Tan ES, Kroon AA. Renal responses to long-term carotid baroreflex activation therapy in patients with drug-resistant hypertension. Hypertension 61: 1334–1339, 2013. - PubMed
-
- Bakris GL, Nadim MK, Haller H, Lovett EG, Schafer JE, Bisognano JD. Baroreflex activation therapy provides durable benefit in patients with resistant hypertension: results of long-term follow-up in the Rheos Pivotal Trial. J Am Soc Hypertens 6: 152–158, 2012. - PubMed
-
- Barrett CJ, Guild SJ, Ramchandra R, Malpas SC. Baroreceptor denervation prevents sympathoinhibition during angiotensin II-induced hypertension. Hypertension 46: 1–5, 2005. - PubMed
-
- Barrett CJ, Ramchandra R, Guild SJ, Lala A, Budgett DM, Malpas SC. What sets the long-term level of renal sympathetic nerve activity: a role for angiotensin II and baroreflexes? Circ Res 92: 1330–1336, 2003. - PubMed
-
- Bisognano JD, Bakris G, Nadim MK, Sanchez L, Kroon AA, Schafer J, de Leeuw PW, Sica DA. Baroreflex activation therapy lowers blood pressure in patients with resistant hypertension: results from the double-blind, randomized, placebo-controlled Rheos Pivotal trial. J Am Coll Cardiol 58: 765–773, 2011. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous