

Impaired Antibody-mediated Protection and Defective IgA B-Cell Memory in Experimental Infection of Adults with Respiratory Syncytial Virus
- PMID: 25730467
- PMCID: PMC4435460
- DOI: 10.1164/rccm.201412-2256OC
Impaired Antibody-mediated Protection and Defective IgA B-Cell Memory in Experimental Infection of Adults with Respiratory Syncytial Virus
Abstract
Rationale: Despite relative antigenic stability, respiratory syncytial virus (RSV) reinfects throughout life. After more than 40 years of research, no effective human vaccine exists and correlates of protection remain poorly defined. Most current vaccine candidates seek to induce high levels of RSV-specific serum neutralizing antibodies, which are associated with reduced RSV-related hospitalization rates in observational studies but may not actually prevent infection.
Objectives: To characterize correlates of protection from infection and the generation of RSV-specific humoral memory to promote effective vaccine development.
Methods: We inoculated 61 healthy adults with live RSV and studied protection from infection by serum and mucosal antibody. We analyzed RSV-specific peripheral blood plasmablast and memory B-cell frequencies and antibody longevity.
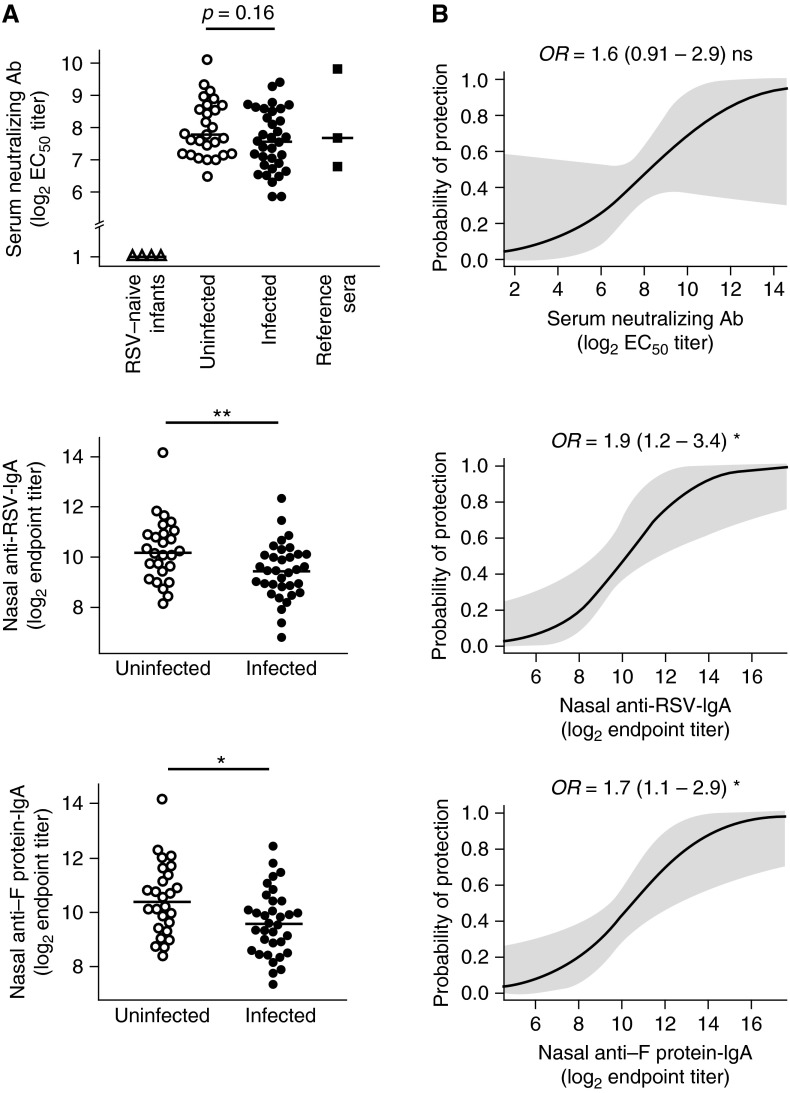
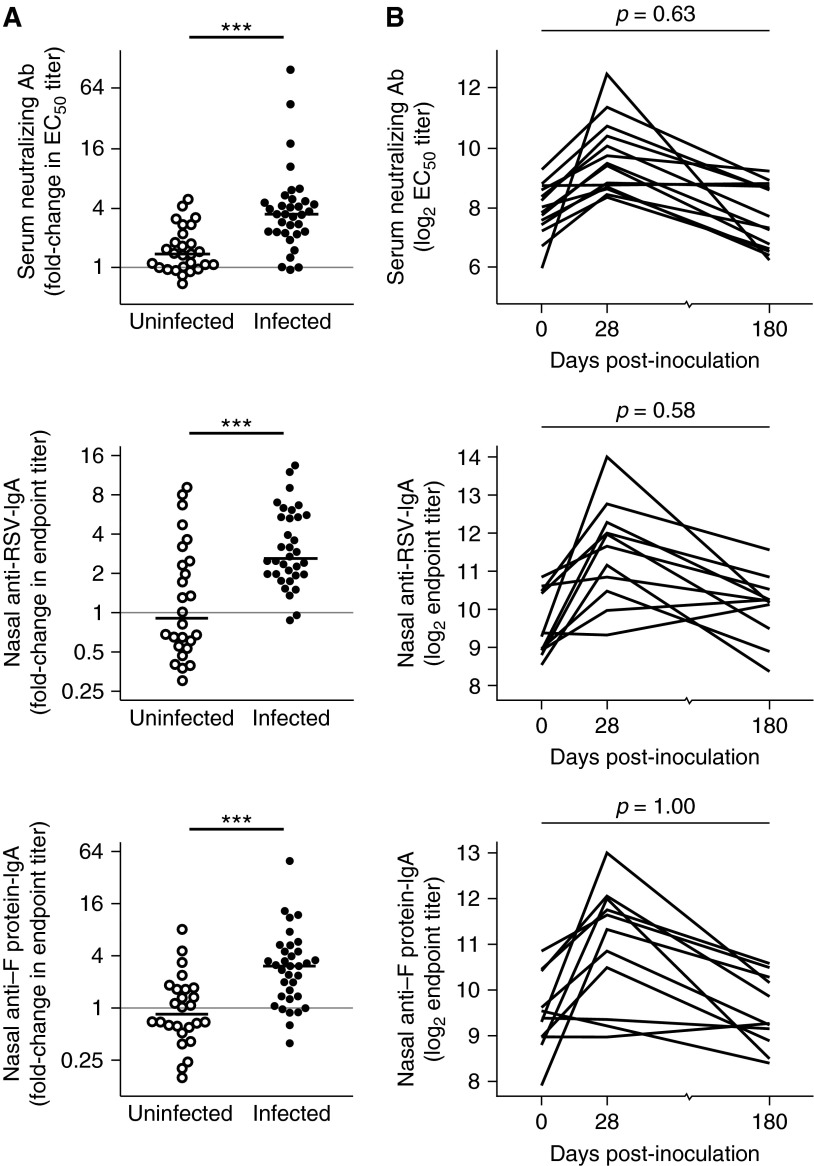
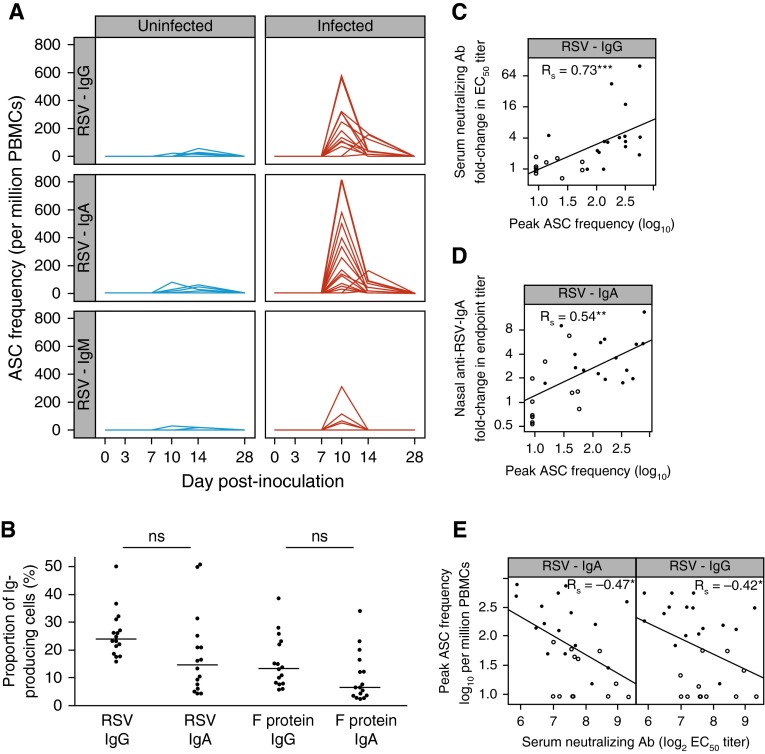
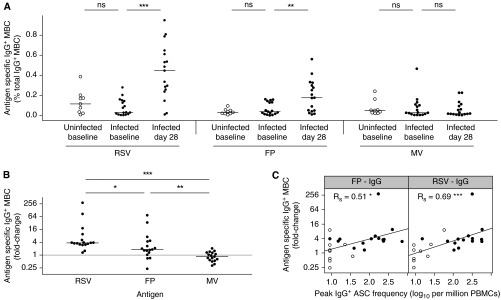
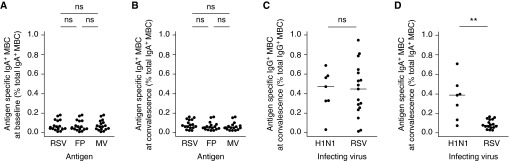
Measurements and main results: Despite moderately high levels of preexisting serum antibody, 34 (56%) became infected, of whom 23 (68%) developed symptomatic colds. Prior RSV-specific nasal IgA correlated significantly more strongly with protection from polymerase chain reaction-confirmed infection than serum neutralizing antibody. Increases in virus-specific antibody titers were variable and transient in infected subjects but correlated with plasmablasts that peaked around Day 10. During convalescence, only IgG (and no IgA) RSV-specific memory B cells were detectable in peripheral blood. This contrasted with natural influenza infection, in which virus-specific IgA memory B cells were readily recovered.
Conclusions: This observed specific defect in IgA memory may partly explain the ability of RSV to cause recurrent symptomatic infections. If so, vaccines able to induce durable RSV-specific IgA responses may be more protective than those generating systemic antibody alone.
Keywords: antibody-secreting cells; immunologic memory; mucosal immunity; nontherapeutic human experimentation; respiratory syncytial virus vaccines.
Figures
Comment in
-
Addressing a challenge with a challenge. Investigating respiratory syncytial virus immunity with the human challenge model.Am J Respir Crit Care Med. 2015 May 1;191(9):975-7. doi: 10.1164/rccm.201503-0471ED. Am J Respir Crit Care Med. 2015. PMID: 25932761 No abstract available.
References
-
- Falsey AR, Hennessey PA, Formica MA, Cox C, Walsh EE. Respiratory syncytial virus infection in elderly and high-risk adults. N Engl J Med. 2005;352:1749–1759. - PubMed
-
- Hall CB, Walsh EE, Long CE, Schnabel KC. Immunity to and frequency of reinfection with respiratory syncytial virus. J Infect Dis. 1991;163:693–698. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
