

Assessment and management of behavioral and psychological symptoms of dementia
- PMID: 25731881
- PMCID: PMC4707529
- DOI: 10.1136/bmj.h369
Assessment and management of behavioral and psychological symptoms of dementia
Abstract
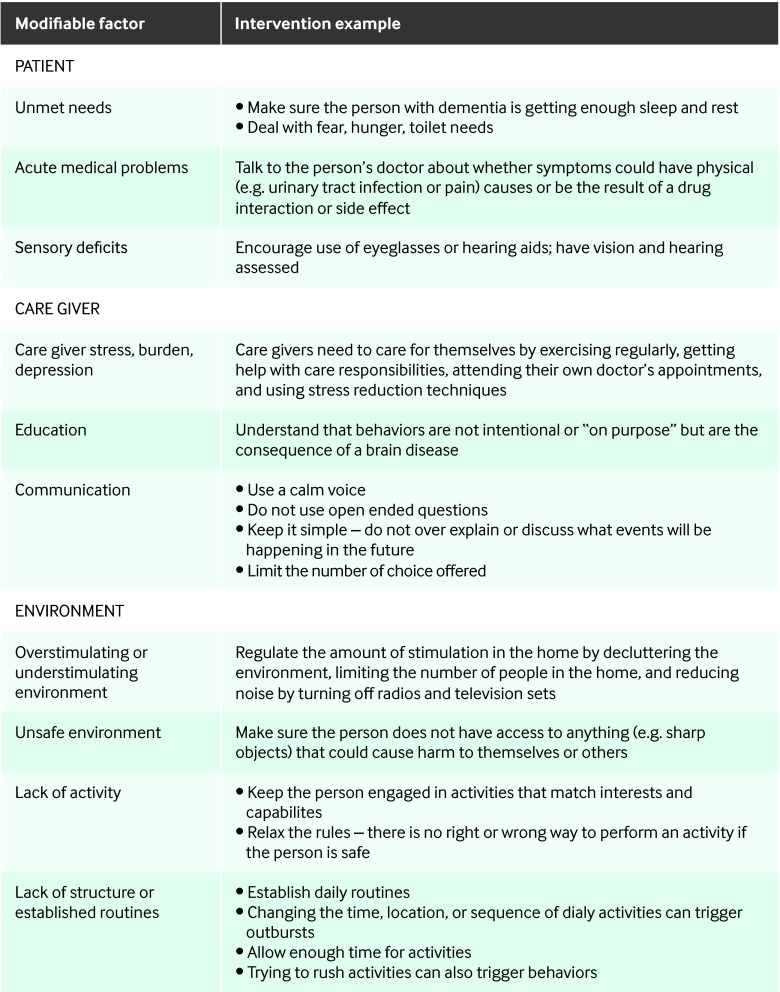
Behavioral and psychological symptoms of dementia include agitation, depression, apathy, repetitive questioning, psychosis, aggression, sleep problems, wandering, and a variety of inappropriate behaviors. One or more of these symptoms will affect nearly all people with dementia over the course of their illness. These symptoms are among the most complex, stressful, and costly aspects of care, and they lead to a myriad of poor patient health outcomes, healthcare problems, and income loss for family care givers. The causes include neurobiologically related disease factors; unmet needs; care giver factors; environmental triggers; and interactions of individual, care giver, and environmental factors. The complexity of these symptoms means that there is no "one size fits all solution," and approaches tailored to the patient and the care giver are needed. Non-pharmacologic approaches should be used first line, although several exceptions are discussed. Non-pharmacologic approaches with the strongest evidence base involve family care giver interventions. Regarding pharmacologic treatments, antipsychotics have the strongest evidence base, although the risk to benefit ratio is a concern. An approach to integrating non-pharmacologic and pharmacologic treatments is described. Finally, the paradigm shift needed to fully institute tailored treatments for people and families dealing with these symptoms in the community is discussed.
© BMJ Publishing Group Ltd 2015.
Conflict of interest statement
Competing interests: We have read and understood the BMJ policy on declaration of interests and declare the following: HCK has received grant support through the National Institutes of Health (NIH) and Department of Veterans Affairs. LNG has received grant support through NIH, Alzheimer’s Association; she is a member on the FallAdvisory Committee for Phillips Lifeline and has received honorariums for various speaking engagements. CGL has received grant support (research or continuing medical education) from the National Institute of Mental Health, the National Institute on Aging, Associated Jewish Federation of Baltimore, Weinberg Foundation, Forest, GlaxoSmithKline, Eisai, Pfizer, AstraZeneca, Lilly, Ortho-McNeil, Bristol-Myers, Novartis, the National Football League (NFL), Elan, and Functional Neuromodulation;he is a consultant or adviser for AstraZeneca, GlaxoSmithKline, Eisai, Novartis, Forest, Supernus, Adlyfe, Takeda, Wyeth, Lundbeck, Merz, Lilly, Pfizer, Genentech, Elan, the NFL Players Association, NFL Benefits Office, Avanir, and Zinfandel and he has received honorariums or travel support from Pfizer, Forest, GlaxoSmithKline, and Health Monitor.
Figures



References
-
- Finkel S, Costae Silva J, Cohen G, Miller S, Sartorius N. Behavioural and psychological signs and symptoms of dementia: a consensus statement on current knowledge and implications for research and treatment. Int Psychogeriatr 1996;8:497-500. - PubMed
-
- Kales HC, Chen P, Blow FC, Welsh DE, Mellow AM. Rates of clinical depression diagnosis, functional impairment, and nursing home placement in coexisting dementia and depression. Am J Geriatr Psychiatry 2005;13:441-9. - PubMed
-
- Yaffe K, Fox P, Newcomer R, Sands L, Lindquist K, Dane K, et al. Patient and caregiver characteristics and nursing home placement in patients with dementia. JAMA 2002;287:2090-7. - PubMed
-
- Wancata J, Windhaber J, Krautgartner M, Alexandrowicz R. The consequences of non-cognitive symptoms of dementia in medical hospital departments. Int J Psychiatry Med 2003;33:257-71. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical