

Outcome of patients admitted with acute coronary syndrome on palliative treatment: insights from the nationwide AMIS Plus Registry 1997-2014
- PMID: 25732032
- PMCID: PMC4360825
- DOI: 10.1136/bmjopen-2014-006218
Outcome of patients admitted with acute coronary syndrome on palliative treatment: insights from the nationwide AMIS Plus Registry 1997-2014
Abstract
Objective: Compliance with guidelines is increasingly used to benchmark the quality of hospital care, however, very little is known on patients admitted with acute coronary syndromes (ACS) and treated palliatively. This study aimed to evaluate the baseline characteristics and outcomes of these patients.
Design: Prospective cohort study.
Setting: Eighty-two Swiss hospitals enrolled patients from 1997 to 2014.
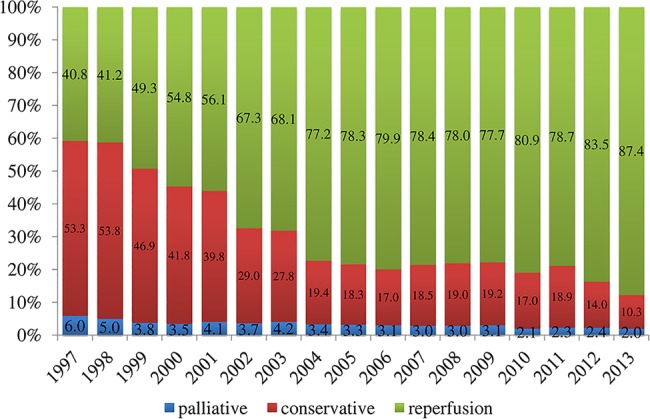
Participants: All patients with ACS enrolled in the AMIS Plus registry (n=45,091) were analysed according to three treatment groups: palliative treatment, defined as use of aspirin and analgesics only and no reperfusion; conservative treatment, defined as any treatment including antithrombotics or anticoagulants, heparins, P2Y12 inhibitors, GPIIb/IIIa but no pharmacological or mechanical reperfusion; and reperfusion treatment (thrombolysis and/or percutaneous coronary intervention during initial hospitalisation). The primary outcome measure was in-hospital mortality and the secondary measure was 1-year mortality.
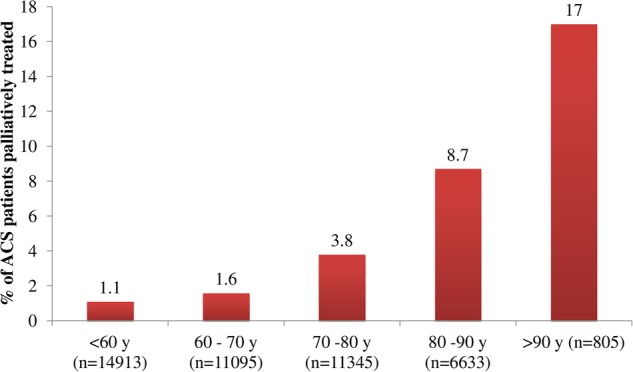
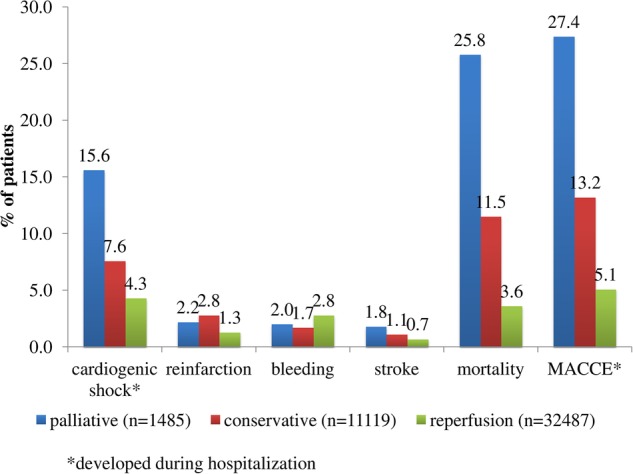
Results: Of the patients, 1485 (3.3%) were palliatively treated, 11,119 (24.7%) were conservatively treated and 32,487 (72.0%) underwent reperfusion therapy. In 1997, 6% of all patients were treated palliatively and this continuously decreased to 2% in 2013. Baseline characteristics of palliative patients differed in comparison with conservatively treated and reperfusion patients in age, gender and comorbidities (all p<0.001). These patients had more in-hospital complications such as postadmission onset of cardiogenic shock (15.6% vs 5.2%; p<0.001), stroke (1.8% vs 0.8%; p=0.001) and a higher in-hospital mortality (25.8% vs 5.6%; p<0.001).The subgroup of patients followed 1 year after discharge (n=8316) had a higher rate of reinfarction (9.2% vs 3.4%; p=0.003) and mortality (14.0% vs 3.5%; p<0.001).
Conclusions: Patients with ACS treated palliatively were older, sicker, with more heart failure at admission and very high in-hospital mortality. While refraining from more active therapy may often constitute the most humane and appropriate approach, we think it is important to also evaluate these patients and include them in registries and outcome evaluations.
Clinical trial number: ClinicalTrials.gov Identifier: NCT01 305 785.
Trial registration: ClinicalTrials.gov NCT01305785.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Figures

References
-
- Witassek F, Schwenkglenks M, Erne P et al. Impact of body mass index on mortality in Swiss hospital patients with ST-elevation myocardial infarction: does an obesity paradox exist? Swiss Med Wkly 2014;144:w13986. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical