

Myocardial viability as integral part of the diagnostic and therapeutic approach to ischemic heart failure
- PMID: 25733105
- PMCID: PMC4490177
- DOI: 10.1007/s12350-015-0096-5
Myocardial viability as integral part of the diagnostic and therapeutic approach to ischemic heart failure
Abstract
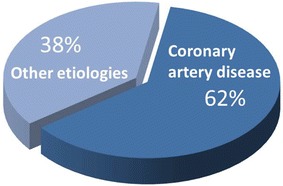
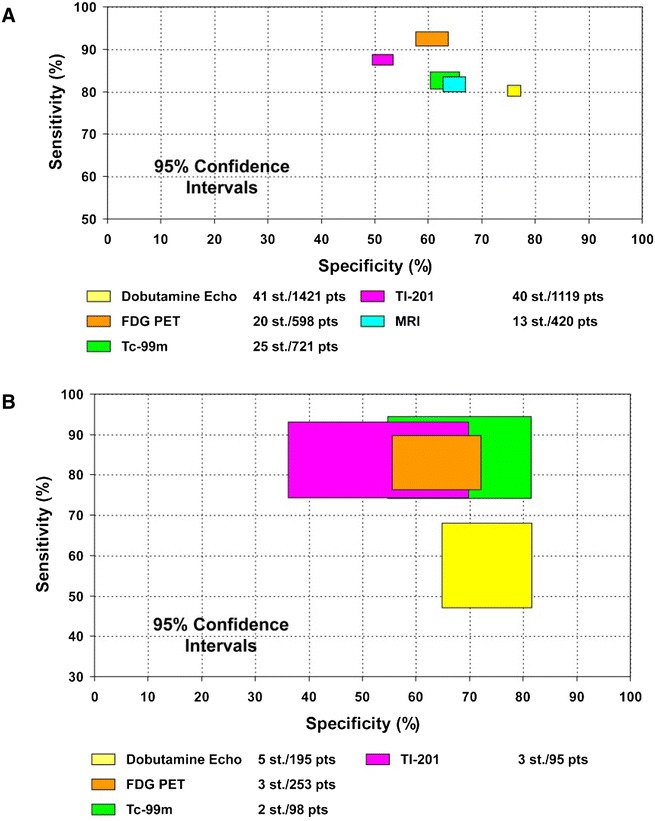
Chronic heart failure is a major public-health problem with a high prevalence, complex treatment, and high mortality. A careful and comprehensive analysis is needed to provide optimal (and personalized) therapy to heart failure patients. The main 4 non-invasive imaging techniques (echocardiography, magnetic resonance imaging, multi-detector-computed tomography, and nuclear imaging) provide information on cardiovascular anatomy and function, which form the basis of the assessment of the pathophysiology underlying heart failure. The selection of imaging modalities depends on the information that is needed for the clinical management of the patients: (1) underlying etiology (ischemic vs non-ischemic); (2) in ischemic patients, need for revascularization should be evaluated (myocardial ischemia/viability?); (3) left ventricular function and shape assessment; (4) presence of significant secondary mitral regurgitation; (5) device therapy with cardiac resynchronization therapy and/or implantable cardiac defibrillator (risk of sudden cardiac death). This review is dedicated to assessment of myocardial viability, however "isolated assessment of myocardial viability" may be clinically not meaningful and should be considered among all those different variables. This complete information will enable personalized treatment of the patient with ischemic heart failure.
Figures
Similar articles
-
Magnetic resonance imaging (MRI) for the assessment of myocardial viability: an evidence-based analysis.Ont Health Technol Assess Ser. 2010;10(15):1-45. Epub 2010 Jul 1. Ont Health Technol Assess Ser. 2010. PMID: 23074392 Free PMC article.
-
Clinical importance of viability assessment in chronic ischemic heart failure.Clin Cardiol. 1996 May;19(5):367-9. doi: 10.1002/clc.4960190507. Clin Cardiol. 1996. PMID: 8723594
-
Alternative Imaging Modalities in Ischemic Heart Failure (AIMI-HF) IMAGE HF Project I-A: study protocol for a randomized controlled trial.Trials. 2013 Jul 16;14:218. doi: 10.1186/1745-6215-14-218. Trials. 2013. PMID: 23866673 Free PMC article. Clinical Trial.
-
[Ischemic cardiomyopathy: possibilities of surgical treatment].Medicina (Kaunas). 2007;43(11):909-17. Medicina (Kaunas). 2007. PMID: 18084150 Review. Lithuanian.
-
Cardiac radionuclide imaging to assess patients with heart failure.Semin Nucl Med. 2014 Jul;44(4):294-313. doi: 10.1053/j.semnuclmed.2014.04.005. Semin Nucl Med. 2014. PMID: 24948152 Review.
Cited by
-
Accelerated (99m)Tc-sestamibi clearance associated with mitochondrial dysfunction and regional left ventricular dysfunction in reperfused myocardium in patients with acute coronary syndrome.EJNMMI Res. 2016 Dec;6(1):41. doi: 10.1186/s13550-016-0196-5. Epub 2016 May 12. EJNMMI Res. 2016. PMID: 27169534 Free PMC article.
-
Evaluation of myocardial viability in old myocardial infarcted patients with CHF: delayed enhancement MRI vs. low-dose dobutamine stress speckle tracking echocardiography.Am J Transl Res. 2016 Sep 15;8(9):3731-3743. eCollection 2016. Am J Transl Res. 2016. PMID: 27725854 Free PMC article.
-
The complex role of cardiovascular imaging in viability testing.Prog Cardiovasc Dis. 2025 Jan-Feb;88:113-125. doi: 10.1016/j.pcad.2024.12.008. Epub 2025 Jan 7. Prog Cardiovasc Dis. 2025. PMID: 39788340 Review.
-
PET/MR: Yet another Tesla?J Nucl Cardiol. 2017 Jun;24(3):1019-1031. doi: 10.1007/s12350-016-0665-2. Epub 2016 Sep 22. J Nucl Cardiol. 2017. PMID: 27659455 Review.
-
Ischaemic and viability testing for guiding PCI are overrated: pros and cons.EuroIntervention. 2024 Mar 18;20(6):e341-e343. doi: 10.4244/EIJ-E-24-00005. EuroIntervention. 2024. PMID: 38506743 Free PMC article. No abstract available.
References
-
- Yancy CW, Jessup M, Bozkurt B, Butler J, Casey DE, Jr, Drazner MH, et al. 2013 ACCF/AHA guideline for the management of heart failure: A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2013;62:e147–e239. doi: 10.1016/j.jacc.2013.05.019. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
