

Morbidity of urologic surgical procedures: an analysis of rates, risk factors, and outcomes
- PMID: 25733265
- PMCID: PMC4349385
- DOI: 10.1016/j.urology.2014.11.034
Morbidity of urologic surgical procedures: an analysis of rates, risk factors, and outcomes
Abstract
Objective: To quantify national complication rates, perioperative outcomes, and predictors for a broad range of urologic procedures to demonstrate background rates and discuss benchmarking.
Methods: Urologic procedures from the National Surgical Quality Improvement Program (2006-2011) were analyzed to identify 30-day rates of 21 complications; outcomes (length of stay, reoperation, and death); and predictors including resident involvement for 18 specific procedures. Multivariate logistic regression models assessed predictors for any complication and for Clavien grade IV or V complication.
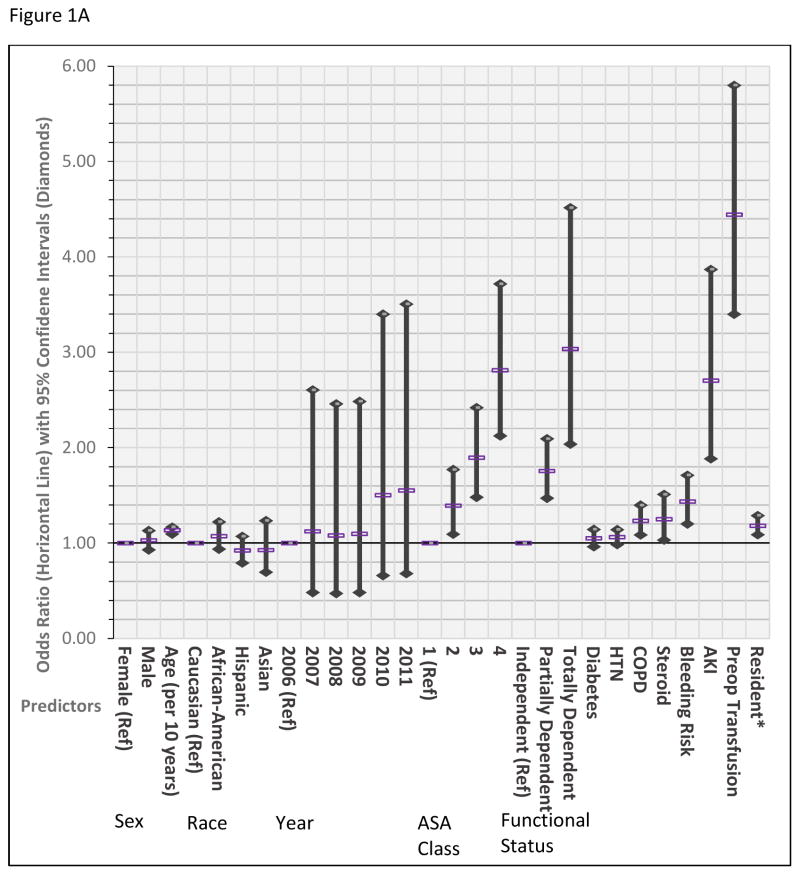
Results: A total of 39,700 procedures were included with abdominopelvic operations more morbid than endoscopic, scrotal, incontinence, or prolapse procedures. Cystectomy had the highest morbidity (10.8 days length of stay and 3.2% mortality), with 56% experiencing any complication followed by nephrectomy (21%), retroperitoneal lymph node dissection (20%), and radical retropubic prostatectomy (19%). Transurethral resection of bladder tumor (11%) and transurethral resection of the prostate (10%) had the highest rates for endoscopic procedures. Older age, American Society of Anesthesiologists class, dependent functional status, acute kidney injury (odds ratio [OR], 2.70 [1.89-3.87]), and ≥5 units preoperative transfusion (OR, 4.44 [3.40-5.80]) were the strongest predictors of any complication. Higher ORs of similar predictors along with chronic obstructive pulmonary disorder (OR, 1.52 [1.21-1.92]) and steroid use (OR, 1.51 [1.07-2.14]) were associated with Clavien grade IV or V complication. Resident involvement increased odds of any complication (OR, 1.18 [1.09-1.29]), mostly for abdominopelvic and urogynecologic procedures, but not Clavien grade IV or V complication (P = .55).
Conclusion: Complication rates of urologic procedures based on the retrospective experience of few surgeons do not allow for appropriate benchmarking. Baseline rates and benchmarks derived from the National Surgical Quality Improvement Program may help hospitals better track deficient areas and improvements in quality of care. Many predictors were similar across procedures, although magnitudes differed, and resident trainees did not impact rates of serious complications (Clavien-Dindo grade IV or V).
Copyright © 2015 Elsevier Inc. All rights reserved.
Figures

Comment in
-
Editorial comment.Urology. 2015 Mar;85(3):559-60. doi: 10.1016/j.urology.2014.11.038. Urology. 2015. PMID: 25733266 No abstract available.
-
Re: Morbidity of Urologic Surgical Procedures: An Analysis of Rates, Risk Factors, and Outcomes.J Urol. 2015 Oct;194(4):1071. doi: 10.1016/j.juro.2015.07.062. Epub 2015 Jul 17. J Urol. 2015. PMID: 26382814 No abstract available.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
