

What to give the patient who has everything? A qualitative study of prescribing for multimorbidity in primary care
- PMID: 25733440
- PMCID: PMC4337307
- DOI: 10.3399/bjgp15X684001
What to give the patient who has everything? A qualitative study of prescribing for multimorbidity in primary care
Abstract
Background: Using clinical guidelines in the management of patients with multimorbidity can lead to the prescription of multiple and sometimes conflicting medications.
Aim: To explore how GPs make decisions when prescribing for multimorbid patients, with a view to informing intervention design.
Design and setting: In-depth qualitative interviews incorporating chart-stimulated recall with purposively sampled GPs in the Republic of Ireland.
Method: Grounded theory analysis with iterative theory development.
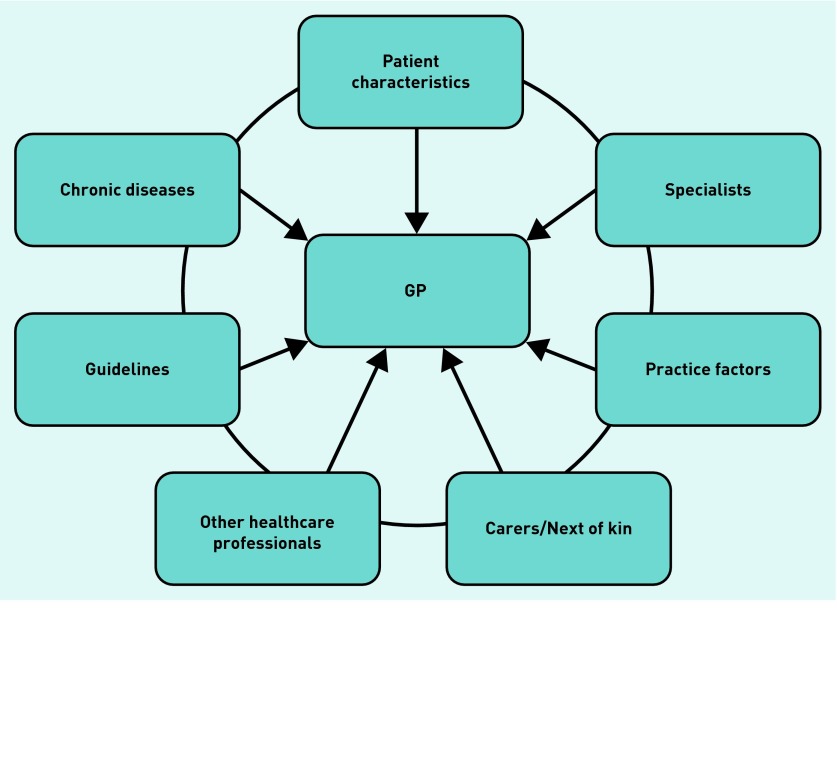
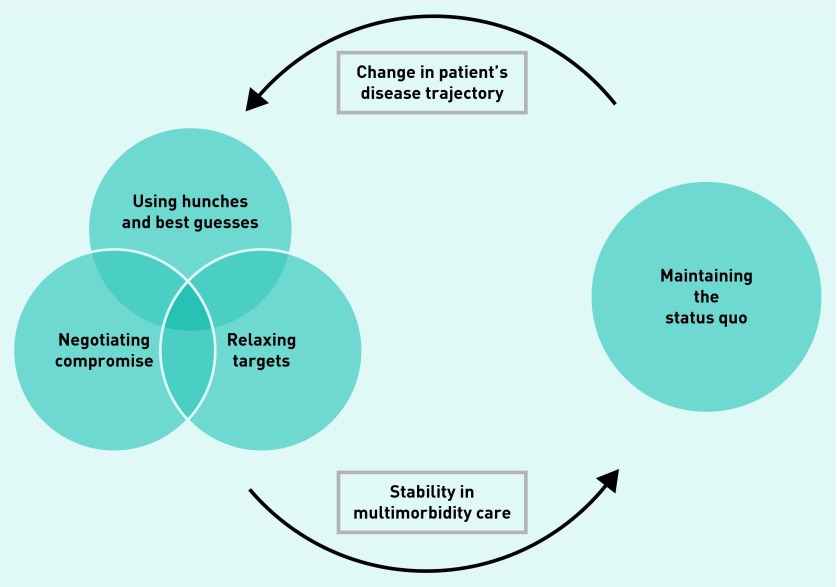
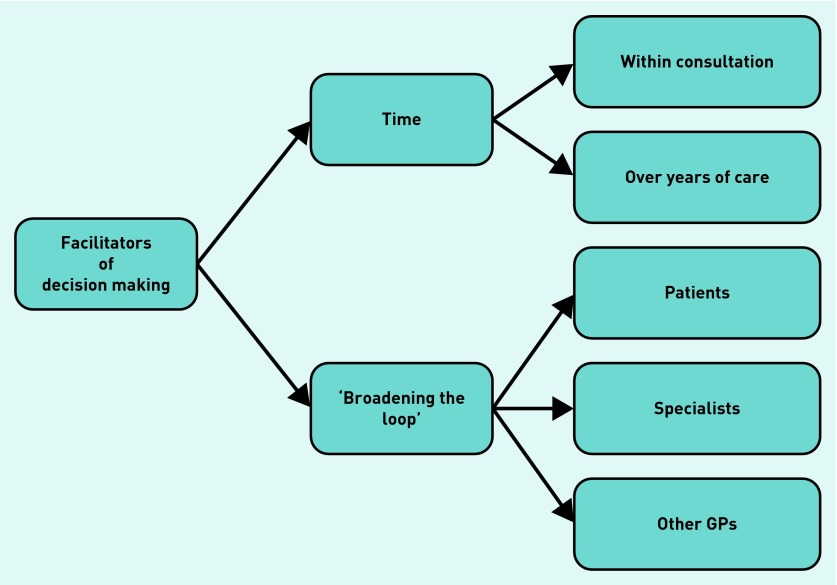
Results: Twenty GPs were interviewed about 51 multimorbid cases. In these cases, GPs integrated information from multiple sources including the patient, specialists, and evidence-based medicine. Difficulties arose when recommendations or preferences conflicted, to which GPs responded by 'satisficing': accepting care that they deemed satisfactory and sufficient for a particular patient. Satisficing was manifest as relaxing targets for disease control, negotiating compromise with the patient, or making 'best guesses' about the most appropriate course of action to take. In multimorbid patients perceived as stable, GPs preferred to 'maintain the status quo' rather than rationalise medications, even in cases with significant polypharmacy. Proactive changes in medications were facilitated by continuity of care, sufficient consultation time, and open lines of communication with the patient, other healthcare professionals, and other GPs.
Conclusion: GPs respond to conflicts in the management of multimorbid patients by making compromises between patient-centred and evidence-based care. These findings will be used to inform interventions that aim to care in multimorbidity.
Keywords: chronic disease; decision making; general practice; medication therapy management; physician’s practice patterns; qualitative research.
© British Journal of General Practice 2015.
Figures
References
-
- Barnett K, Mercer SW, Norbury M, et al. Epidemiology of multimorbidity and implications for health care, research, and medical education: a cross-sectional study. Lancet. 2012;380:37–43. - PubMed
-
- Marengoni A, Angleman S, Melis R, et al. Aging with multimorbidity: a systematic review of the literature. Ageing Res Rev. 2011;10:430–439. - PubMed
-
- Glynn LG, Valderas JM, Healy P, et al. The prevalence of multimorbidity in primary care and its effect on health care utilization and cost. Fam Pract. 2011;28:516–523. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical