

Cause of Death in Patients with Reduced Kidney Function
- PMID: 25733525
- PMCID: PMC4587695
- DOI: 10.1681/ASN.2014070714
Cause of Death in Patients with Reduced Kidney Function
Abstract
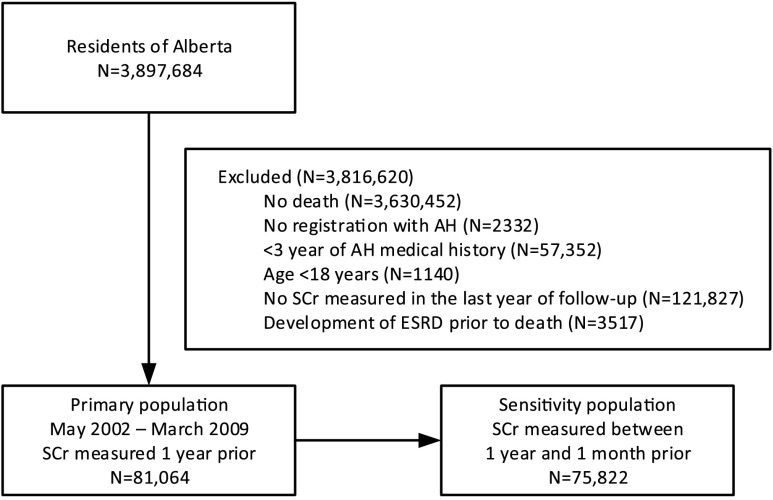
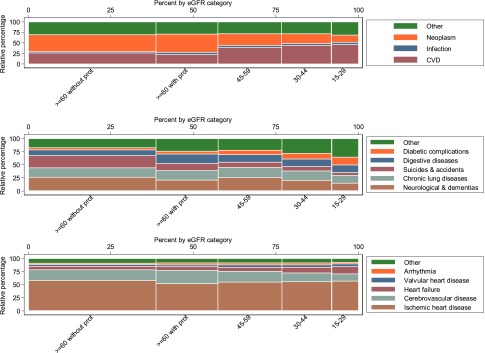
Information on common causes of death in people with CKD is limited. We hypothesized that, as eGFR declines, cardiovascular mortality and mortality from infection account for increasing proportions of deaths. We calculated eGFR using the CKD Epidemiology Collaboration equation for residents of Alberta, Canada who died between 2002 and 2009. We used multinomial logistic regression to estimate unadjusted and age- and sex-adjusted differences in the proportions of deaths from each cause according to the severity of CKD. Cause of death was classified as cardiovascular, infection, cancer, other, or not reported using International Classification of Diseases codes. Among 81,064 deaths, the most common cause was cancer (31.9%) followed by cardiovascular disease (30.2%). The most common cause of death for those with eGFR≥60 ml/min per 1.73 m(2) and no proteinuria was cancer (38.1%); the most common cause of death for those with eGFR<60 ml/min per 1.73 m(2) was cardiovascular disease. The unadjusted proportion of patients who died from cardiovascular disease increased as eGFR decreased (20.7%, 36.8%, 41.2%, and 43.7% of patients with eGFR≥60 [with proteinuria], 45-59.9, 30-44.9, and 15-29.9 ml/min per 1.73 m(2), respectively). The proportions of deaths from heart failure and valvular disease specifically increased with declining eGFR along with the proportions of deaths from infectious and other causes, whereas the proportion of deaths from cancer decreased. In conclusion, we found an inverse association between eGFR and specific causes of death, including specific types of cardiovascular disease, infection, and other causes, in this cohort.
Keywords: CKD; GFR; cardiovascular disease; epidemiology and outcomes; mortality.
Copyright © 2015 by the American Society of Nephrology.
Figures
Comment in
-
Not All Deaths in CKD Are from a Broken Heart.J Am Soc Nephrol. 2015 Oct;26(10):2307-8. doi: 10.1681/ASN.2015050531. Epub 2015 Jun 4. J Am Soc Nephrol. 2015. PMID: 26045087 Free PMC article. No abstract available.
References
-
- Lozano R, Naghavi M, Foreman K, Lim S, Shibuya K, Aboyans V, Abraham J, Adair T, Aggarwal R, Ahn SY, Alvarado M, Anderson HR, Anderson LM, Andrews KG, Atkinson C, Baddour LM, Barker-Collo S, Bartels DH, Bell ML, Benjamin EJ, Bennett D, Bhalla K, Bikbov B, Bin Abdulhak A, Birbeck G, Blyth F, Bolliger I, Boufous S, Bucello C, Burch M, Burney P, Carapetis J, Chen H, Chou D, Chugh SS, Coffeng LE, Colan SD, Colquhoun S, Colson KE, Condon J, Connor MD, Cooper LT, Corriere M, Cortinovis M, de Vaccaro KC, Couser W, Cowie BC, Criqui MH, Cross M, Dabhadkar KC, Dahodwala N, De Leo D, Degenhardt L, Delossantos A, Denenberg J, Des Jarlais DC, Dharmaratne SD, Dorsey ER, Driscoll T, Duber H, Ebel B, Erwin PJ, Espindola P, Ezzati M, Feigin V, Flaxman AD, Forouzanfar MH, Fowkes FGR, Franklin R, Fransen M, Freeman MK, Gabriel SE, Gakidou E, Gaspari F, Gillum RF, Gonzalez-Medina D, Halasa YA, Haring D, Harrison JE, Havmoeller R, Hay RJ, Hoen B, Hotez PJ, Hoy D, Jacobsen KH, James SL, Jasrasaria R, Jayaraman S, Johns N, Karthikeyan G, Kassebaum N, Keren A, Khoo JP, Knowlton LM, Kobusingye O, Koranteng A, Krishnamurthi R, Lipnick M, Lipshultz SE, Ohno SL, Mabweijano J, MacIntyre MF, Mallinger L, March L, Marks GB, Marks R, Matsumori A, Matzopoulos R, Mayosi BM, McAnulty JH, McDermott MM, McGrath J, Mensah GA, Merriman TR, Michaud C, Miller M, Miller TR, Mock C, Mocumbi AO, Mokdad AA, Moran A, Mulholland K, Nair MN, Naldi L, Narayan KM, Nasseri K, Norman P, O’Donnell M, Omer SB, Ortblad K, Osborne R, Ozgediz D, Pahari B, Pandian JD, Rivero AP, Padilla RP, Perez-Ruiz F, Perico N, Phillips D, Pierce K, Pope CA, 3rd, Porrini E, Pourmalek F, Raju M, Ranganathan D, Rehm JT, Rein DB, Remuzzi G, Rivara FP, Roberts T, De León FR, Rosenfeld LC, Rushton L, Sacco RL, Salomon JA, Sampson U, Sanman E, Schwebel DC, Segui-Gomez M, Shepard DS, Singh D, Singleton J, Sliwa K, Smith E, Steer A, Taylor JA, Thomas B, Tleyjeh IM, Towbin JA, Truelsen T, Undurraga EA, Venketasubramanian N, Vijayakumar L, Vos T, Wagner GR, Wang M, Wang W, Watt K, Weinstock MA, Weintraub R, Wilkinson JD, Woolf AD, Wulf S, Yeh PH, Yip P, Zabetian A, Zheng ZJ, Lopez AD, Murray CJ, AlMazroa MA, Memish ZA: Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 380: 2095–2128, 2012 - PMC - PubMed
-
- Couser WG, Remuzzi G, Mendis S, Tonelli M: The contribution of chronic kidney disease to the global burden of major noncommunicable diseases. Kidney Int 80: 1258–1270, 2011 - PubMed
-
- Fried LF, Katz R, Sarnak MJ, Shlipak MG, Chaves PHM, Jenny NS, Stehman-Breen C, Gillen D, Bleyer AJ, Hirsch C, Siscovick D, Newman AB: Kidney function as a predictor of noncardiovascular mortality. J Am Soc Nephrol 16: 3728–3735, 2005 - PubMed
-
- James MT, Quan H, Tonelli M, Manns BJ, Faris P, Laupland KB, Hemmelgarn BR, Alberta Kidney Disease Network : CKD and risk of hospitalization and death with pneumonia. Am J Kidney Dis 54: 24–32, 2009 - PubMed
-
- Marks A, Macleod C, McAteer A, Murchie P, Fluck N, Smith WCS, Prescott GJ, Clark LE, Ali T, Black C: Chronic kidney disease, a useful trigger for proactive primary care? Mortality results from a large U.K. cohort. Fam Pract 30: 282–289, 2013 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
