

The NorthStar Ambulatory Assessment in Duchenne muscular dystrophy: considerations for the design of clinical trials
- PMID: 25733532
- PMCID: PMC4752678
- DOI: 10.1136/jnnp-2014-309405
The NorthStar Ambulatory Assessment in Duchenne muscular dystrophy: considerations for the design of clinical trials
Abstract
Objective: With the emergence of experimental therapies for Duchenne muscular dystrophy (DMD), it is fundamental to understand the natural history of this disorder to properly design clinical trials. The aims of this study were to assess the effects produced on motor function by different DMD genotypes and early initiation of glucocorticoids.
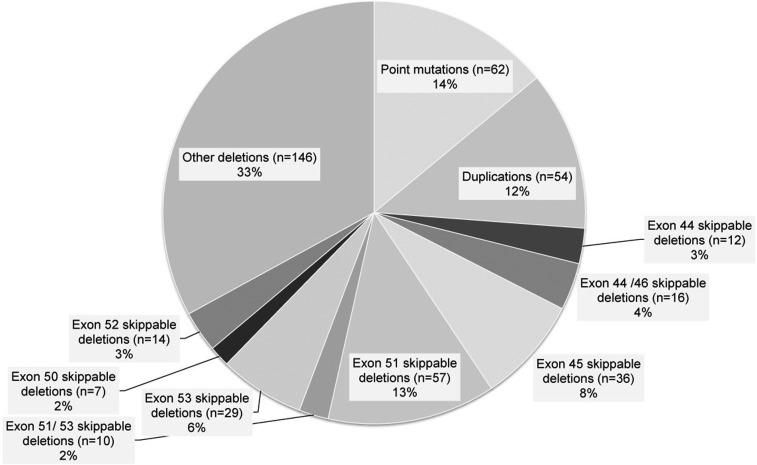
Methods: Through the NorthStar Network, standardised clinical data including the NorthStar Ambulatory Assessment score (NSAA) on 513 ambulant UK boys with DMD were analysed from 2004 to 2012. For the analysis of the genetic subpopulation, we also included data from 172 Italian boys with DMD. NSAA raw scores were converted into linear scores.
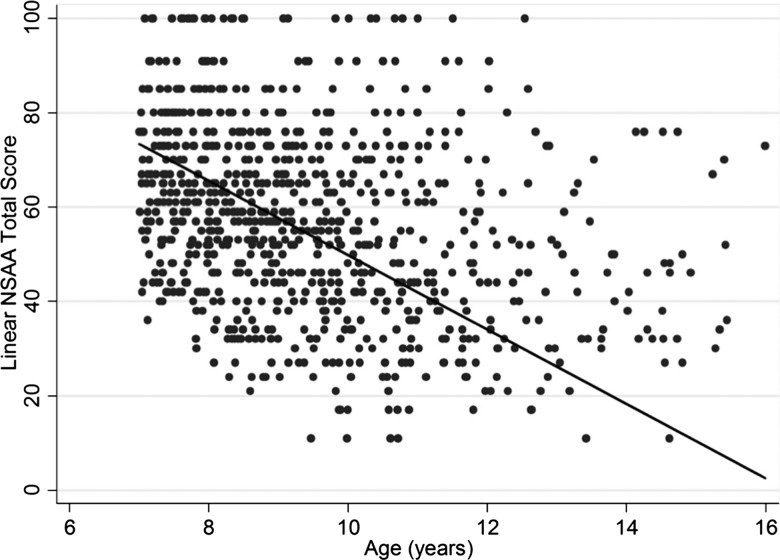
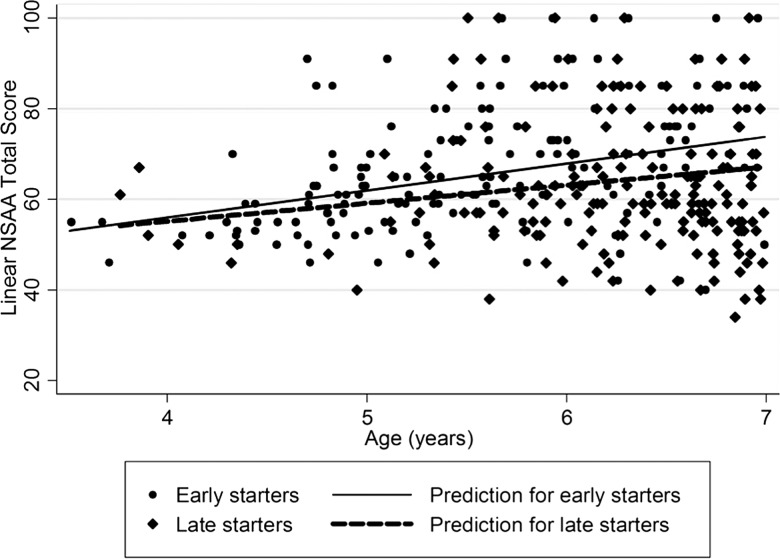
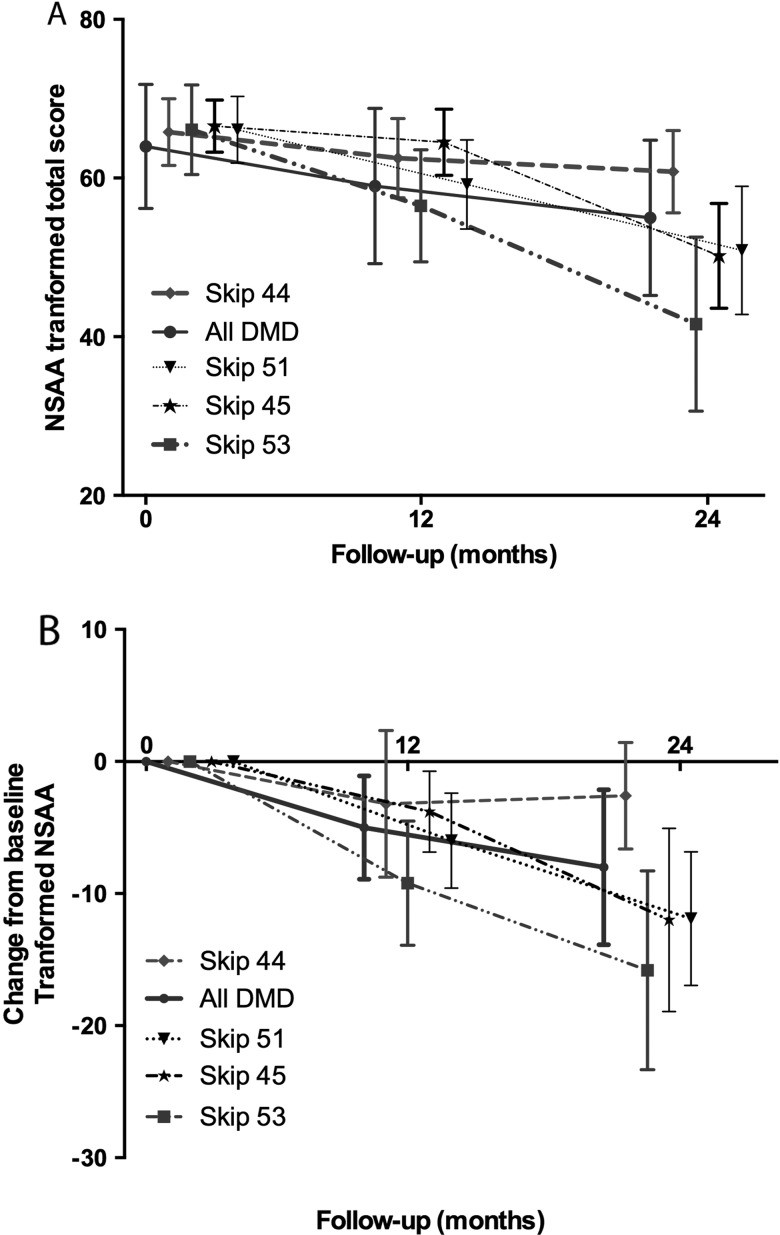
Results: On the linearised NSAA, we observed an average decline of 8 units/year (4 units on raw NSAA analysis) after age 7. The median age at loss of ambulation (LOA) was 13 years (95% CI 12.1 to 13.5); 2 years prior to LOA, the estimated mean linearised NSAA score was 42/100 (13/34 raw scale). Starting glucocorticoids between 3 and 5 years conferred an additional gain in motor function of 3 units/year (1.3 raw units) up to age 7. When analysing the effect of genotype in the UK and Italian cumulative cohorts, individuals with deletions amenable to exons 44 and 46 skipping declined at a slower rate over 2 years (9 units (4 raw units), p<0.001), while 53 and 51 skippable deletions showed a faster decline of 14 (4.5; p<0.001) and 5 linearised units (2.4 NSAA units; p=0.02), respectively.
Conclusions: Our study provides a novel insight on the current natural history of DMD, which will be instrumental for the design of future clinical trials.
Keywords: MUSCULAR DYSTROPHY; NEUROMUSCULAR.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://www.bmj.com/company/products-services/rights-and-licensing/
Figures
References
-
- Cirak S, Arechavala-Gomeza V, Guglieri M, et al. . Exon skipping and dystrophin restoration in patients with Duchenne muscular dystrophy after systemic phosphorodiamidate morpholino oligomer treatment: an open-label, phase 2, dose-escalation study. Lancet 2011;378:595–605. 10.1016/S0140-6736(11)60756-3 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical