

Pneumonia in childhood and impaired lung function in adults: a longitudinal study
- PMID: 25733757
- PMCID: PMC4379462
- DOI: 10.1542/peds.2014-3060
Pneumonia in childhood and impaired lung function in adults: a longitudinal study
Abstract
Background: Diminished lung function and increased prevalence of asthma have been reported in children with a history of early lower respiratory illnesses (LRIs), including pneumonia. Whether these associations persist up to adulthood has not been established.
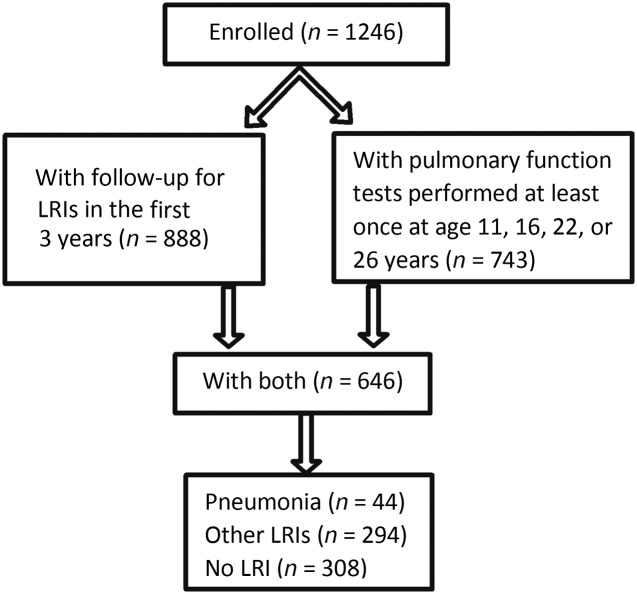
Methods: As part of the prospective Tucson Children's Respiratory Study, LRIs during the first 3 years of life were ascertained by pediatricians. Spirometry was performed at ages 11, 16, 22, and 26 years. The occurrence of asthma/wheeze during the previous year was ascertained at ages 11, 13, 16, 18, 22, 24, 26, and 29 years. Longitudinal random effects models and generalized estimating equations were used to assess the relation of LRIs to lung function and asthma.
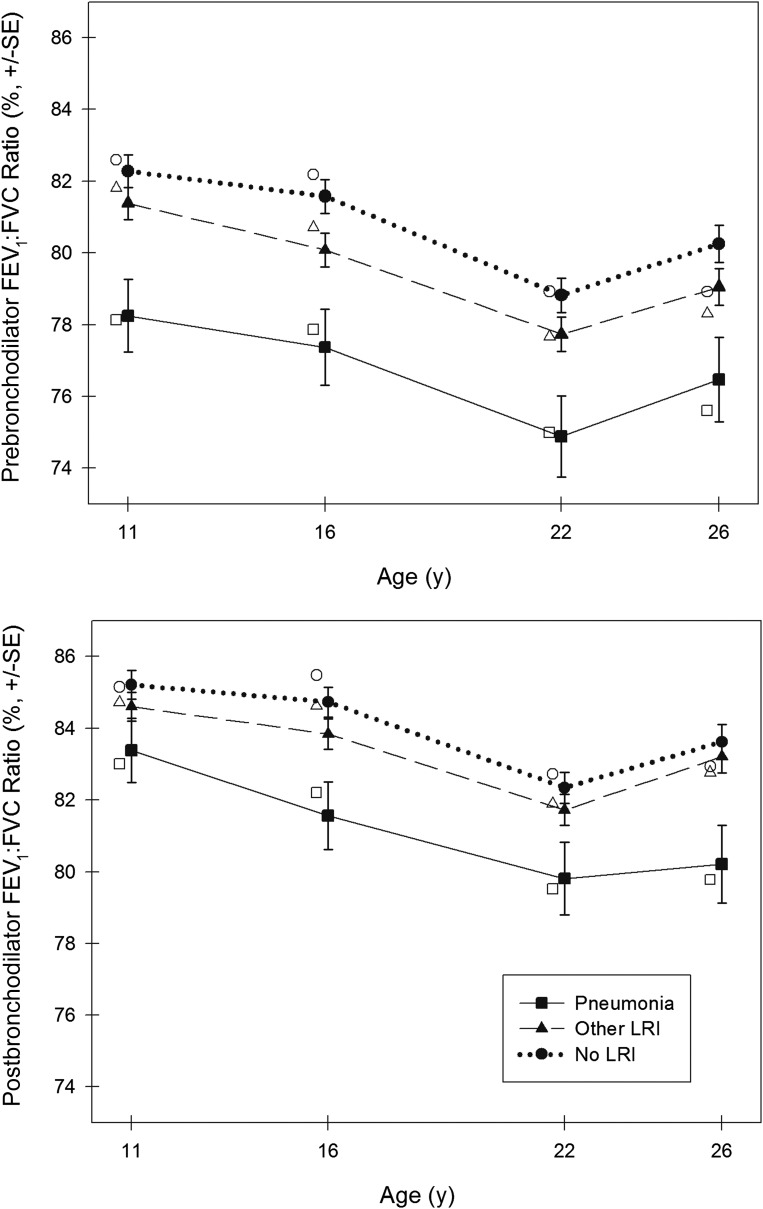
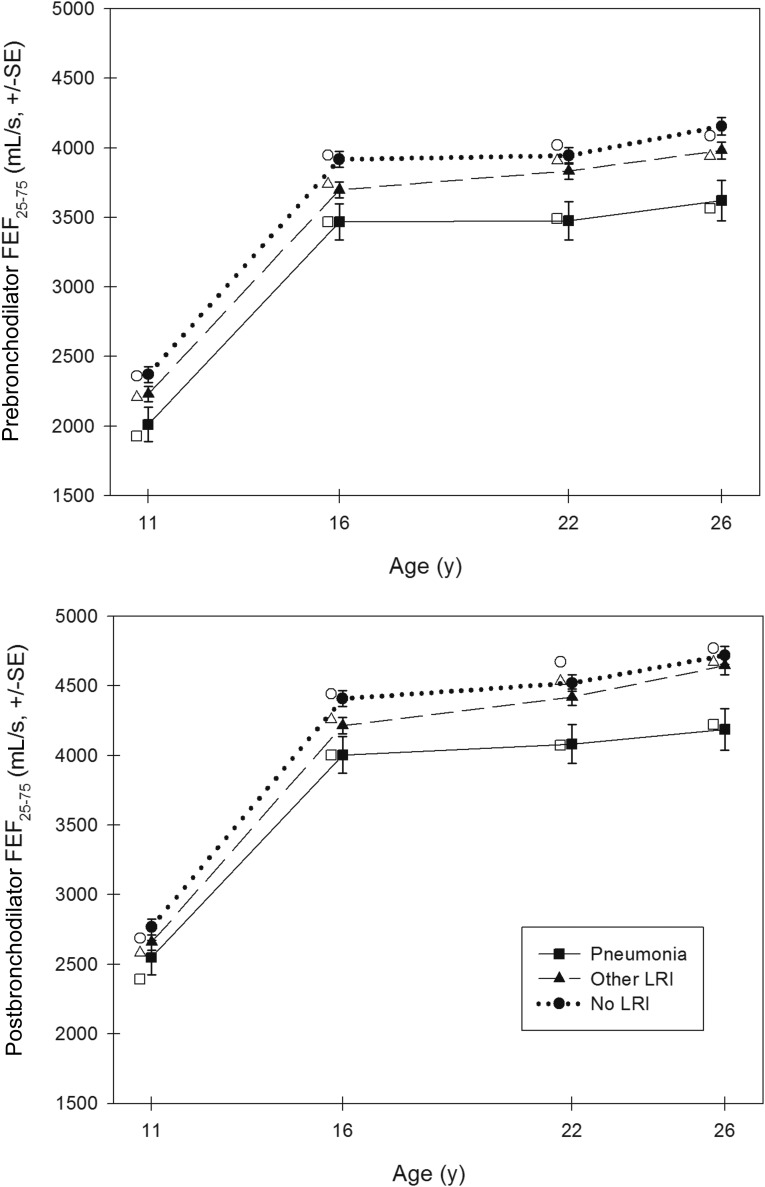
Results: Compared with participants without early-life LRIs, those with pneumonia had the most severe subsequent lung function impairment, with mean ± SE deficits of -3.9% ± 0.9% (P < .001) and -2.5% ± 0.8% (P = .001) for pre- and post-bronchodilator FEV1:FVC ratio from age 11 to 26 years, respectively. Pneumonia was associated with increased risk for asthma (odds ratio [OR]: 1.95; 95% confidence interval [CI]: 1.11-3.44) and wheeze (OR: 1.94; 95% CI: 1.28-2.95) over the same age range. Early non-pneumonia LRIs were associated with mildly impaired pre-bronchodilator FEV1 (-62.8 ± 27.9 mL, P = .024) and FEV1:FVC ratio (-1.1 ± 0.5%, P = .018), and wheeze (OR: 1.37; 95% CI: 1.09-1.72).
Conclusions: Early pneumonia is associated with asthma and impaired airway function, which is partially reversible with bronchodilators and persists into adulthood. Early pneumonia may be a major risk factor for adult chronic obstructive pulmonary disease.
Keywords: asthma; early childhood pneumonia; lung function.
Copyright © 2015 by the American Academy of Pediatrics.
Figures
Comment in
-
Long-term effects of childhood chest infections.Arch Dis Child. 2015 Jul;100(7):636. doi: 10.1136/archdischild-2015-308956. Epub 2015 May 28. Arch Dis Child. 2015. PMID: 26023004 No abstract available.
References
-
- Castro-Rodríguez JA, Holberg CJ, Wright AL, et al. Association of radiologically ascertained pneumonia before age 3 yr with asthmalike symptoms and pulmonary function during childhood: a prospective study. Am J Respir Crit Care Med. 1999;159(6):1891–1897 - PubMed
-
- Kusel MM, Kebadze T, Johnston SL, Holt PG, Sly PD. Febrile respiratory illnesses in infancy and atopy are risk factors for persistent asthma and wheeze. Eur Respir J. 2012;39(4):876–882 - PubMed
-
- Anderson HR, Bland JM, Peckham CS. Risk factors for asthma up to 16 years of age: evidence from a national cohort study. Chest. 1987;91(6 suppl):127S–130S - PubMed
-
- Korppi M, Kuikka L, Reijonen T, Remes K, Juntunen-Backman K, Launiala K. Bronchial asthma and hyperreactivity after early childhood bronchiolitis or pneumonia. An 8-year follow-up study. Arch Pediatr Adolesc Med. 1994;148(10):1079–1084 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
