

Higher human T-lymphotropic virus type 1 subtype C proviral loads are associated with bronchiectasis in indigenous australians: results of a case-control study
- PMID: 25734096
- PMCID: PMC4324180
- DOI: 10.1093/ofid/ofu023
Higher human T-lymphotropic virus type 1 subtype C proviral loads are associated with bronchiectasis in indigenous australians: results of a case-control study
Abstract
Background: We previously suggested that infection with the human T-lymphotropic virus type 1 (HTLV-1) subtype C is associated with bronchiectasis among Indigenous Australians. Bronchiectasis might therefore result from an HTLV-1-mediated inflammatory process that is typically associated with a high HTLV-1 proviral load (PVL). Human T-lymphotropic virus type 1 PVL have not been reported for Indigenous Australians.
Methods: Thirty-six Indigenous adults admitted with bronchiectasis from June 1, 2008, to December 31, 2009 were prospectively recruited and matched by age, sex, and ethno-geographic origin to 36 controls. Case notes and chest high-resolution computed tomographs were reviewed, and pulmonary injury scores were calculated. A PVL assay for the HTLV-1c subtype that infects Indigenous Australians was developed and applied to this study. Clinical, radiological, and virological parameters were compared between groups and according to HTLV-1 serostatus.
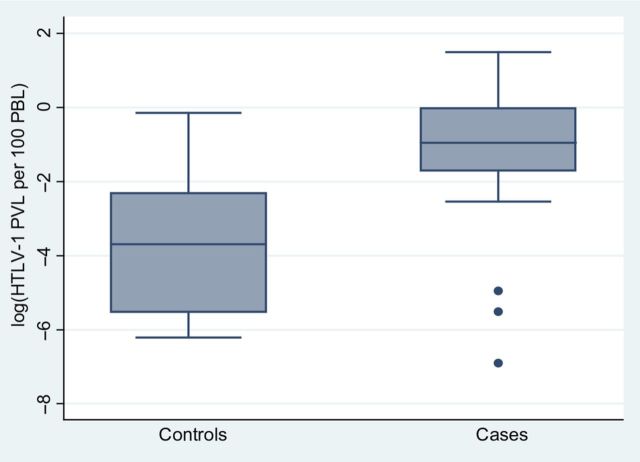
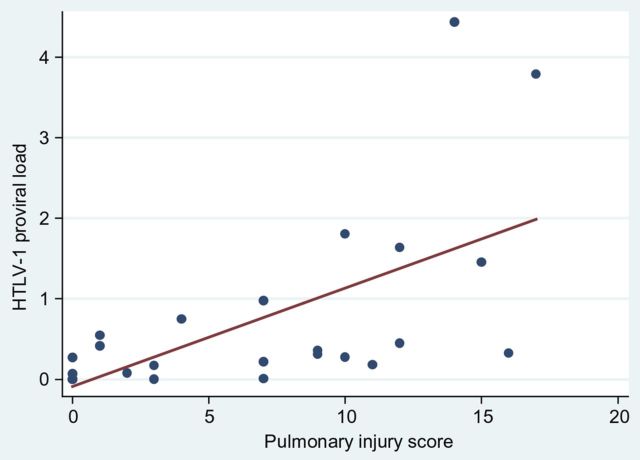
Results: Human T-lymphotropic virus type 1 infection was the main predictor of bronchiectasis in a multivariable model (adjusted risk ratio [aRR], 1.84; 95% confidence interval [CI], 1.19-2.84; P = .006). Moreover, the median HTLV-1c PVL (interquartile range) for cases was >100-fold that of controls (cases, 0.319 [0.007, 0.749]; controls, 0.003 [0.000, 0.051] per 100 peripheral blood lymphocytes; P = .007), and HTLV-1c PVL were closely correlated with radiologically determined pulmonary injury scores (Spearman's rho = 0.7457; P = .0000). Other predictors of bronchiectasis were positive Strongyloides serology (aRR, 1.69; 95% CI, 1.13-2.53) and childhood skin infections (aRR, 1.62; 95% CI, 1.07-2.44). Bronchiectasis was the major predictor of death (aRR, 2.71; 95% CI, 1.36-5.39; P = .004).
Conclusions: These data strongly support an etiological association between HTLV-1 infection and bronchiectasis in a socially disadvantaged population at risk of recurrent lower respiratory tract infections.
Keywords: Australia; HTLV-1; HTLV-1 proviral load; Indigenous; Strongyloides stercoralis; bronchiectasis; pulmonary disease.
Figures
References
-
- Bastian I, Hinuma Y, Doherty RR. HTLV-1 among Northern Territory Aborigines. Med J Aust. 1993;159:12–6. - PubMed
-
- Bastian I. Darwin: University of Sydney; 1996. HTLV-1 studies in the Northern Territory. PhD Thesis.
-
- Verdonck K, Gonzalez E, Van Dooren S, et al. Human T-lymphotropic virus 1: recent knowledge about an ancient infection. Lancet Infect Dis. 2007;7:266–81. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
