

Standardized electrolyte supplementation and fluid management improves survival during amphotericin therapy for cryptococcal meningitis in resource-limited settings
- PMID: 25734140
- PMCID: PMC4281785
- DOI: 10.1093/ofid/ofu070
Standardized electrolyte supplementation and fluid management improves survival during amphotericin therapy for cryptococcal meningitis in resource-limited settings
Abstract
Background: Amphotericin B is the preferred treatment for cryptococcal meningitis, but it has cumulative severe side effects, including nephrotoxicity, hypokalemia, and hypomagnesemia. Amphotericin-induced severe hypokalemia may predispose the patient to cardiac arrhythmias and death, and there is very little data available regarding these toxicities in resource-limited settings. We hypothesized that standardized electrolyte management during amphotericin therapy is essential to minimize toxicity and optimize survival in sub-Saharan Africa.
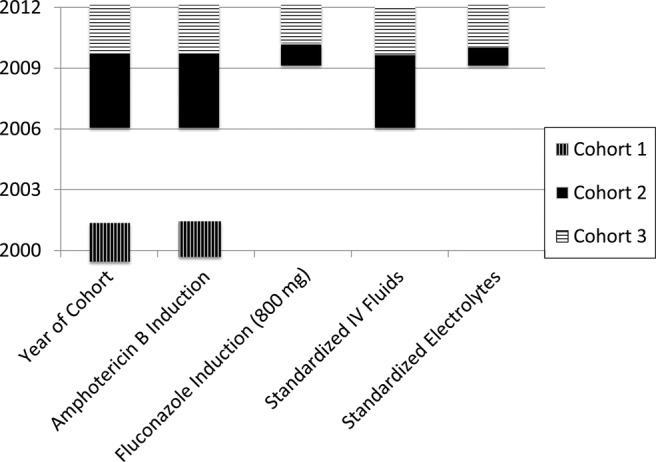
Methods: Human immunodeficiency virus-infected, antiretroviral therapy naive adults with cryptococcal meningitis were prospectively enrolled at Mulago Hospital in Kampala, Uganda in 3 sequential cohorts with amphotericin B deoxycholate induction treatment. Intravenous fluid use was intermittent in 2001-2002, and universal in 2006-2012. In 2001-2009, serum potassium (K(+)) was monitored on days 1, 7, and 14 of treatment with replacement (K(+), Mg(2+)) per clinician discretion. In 2011-2012, K(+) was measured on days 1, 5, and approximately every 48 hours thereafter with universal electrolyte (K(+), Mg(2+)) supplementation and standardized replacement. Clinical outcomes were retrospectively compared between fluid and electrolyte management strategies.
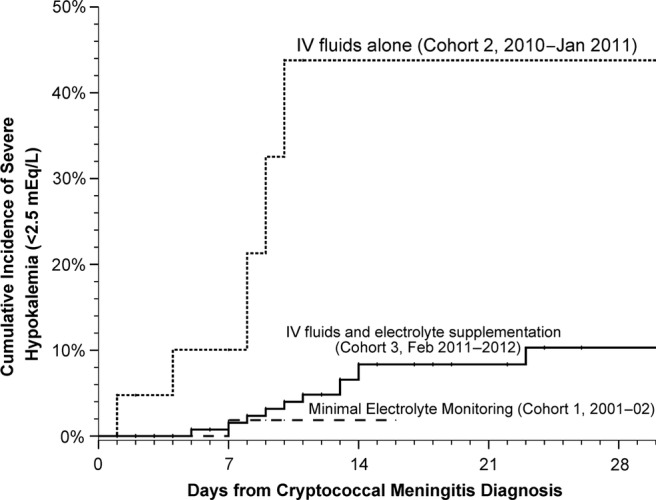
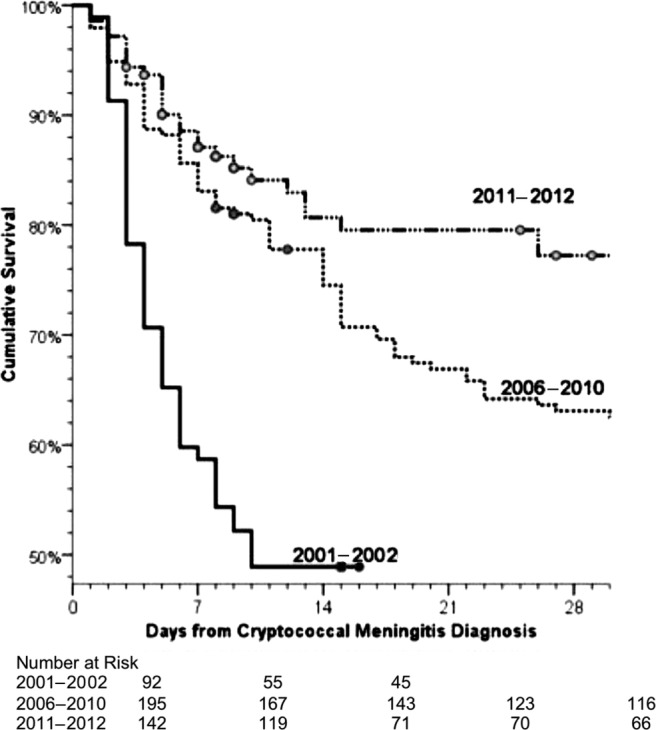
Results: With limited intravenous fluids, the 14-day survival was 49% in 2001-2002. With universal intravenous fluids, the 30-day survival improved to 62% in 2006-2010 (P = .003). In 2011-2012, with universal supplementation of fluids and electrolytes, 30-day cumulative survival improved to 78% (P = .021 vs 2006-2010 cohort). The cumulative incidence of severe hypokalemia (<2.5 mEq/L) decreased from 38% in 2010 to 8.5% in 2011-2012 with universal supplementation (P < .001).
Conclusions: Improved survival was seen in a resource-limited setting with proactive fluid and electrolyte management (K(+), Mg(2+)), as part of comprehensive amphotericin-based cryptococcal therapy.
Keywords: HIV/AIDS; amphotericin; cryptococcal meningitis; potassium; side effect.
Figures
Similar articles
-
Management of cryptococcal meningitis in HIV-infected patients: Experience from western India.Indian J Sex Transm Dis AIDS. 2010 Jan;31(1):22-6. doi: 10.4103/0253-7184.68996. Indian J Sex Transm Dis AIDS. 2010. PMID: 21808432 Free PMC article.
-
[A clinical study of 26 cases of cryptococcal meningitis].Zhonghua Nei Ke Za Zhi. 2002 Aug;41(8):541-3. Zhonghua Nei Ke Za Zhi. 2002. PMID: 12421503 Chinese.
-
High Mortality in HIV-Associated Cryptococcal Meningitis Patients Treated With Amphotericin B-Based Therapy Under Routine Care Conditions in Africa.Open Forum Infect Dis. 2018 Oct 23;5(11):ofy267. doi: 10.1093/ofid/ofy267. eCollection 2018 Nov. Open Forum Infect Dis. 2018. PMID: 30488038 Free PMC article.
-
HIV-Associated Cryptococcal Disease in Resource-Limited Settings: A Case for "Prevention Is Better Than Cure"?J Fungi (Basel). 2017 Dec 2;3(4):67. doi: 10.3390/jof3040067. J Fungi (Basel). 2017. PMID: 29371581 Free PMC article. Review.
-
Overview: treatment of cryptococcal meningitis.Rev Infect Dis. 1990 Mar-Apr;12 Suppl 3:S338-48. doi: 10.1093/clinids/12.supplement_3.s338. Rev Infect Dis. 1990. PMID: 2184512 Review.
Cited by
-
Ambulatory induction phase treatment of cryptococcal meningitis in HIV integrated primary care clinics, Yangon, Myanmar.BMC Infect Dis. 2021 Apr 21;21(1):375. doi: 10.1186/s12879-021-06049-z. BMC Infect Dis. 2021. PMID: 33882845 Free PMC article.
-
Cryptococcal Meningitis: Diagnosis and Management Update.Curr Trop Med Rep. 2015 Jun 1;2(2):90-99. doi: 10.1007/s40475-015-0046-y. Curr Trop Med Rep. 2015. PMID: 26279970 Free PMC article.
-
Using single-dose liposomal amphotericin B for cryptococcal meningitis induction therapy: nurse pearls and practical perspectives.Wellcome Open Res. 2024 Oct 17;9:253. doi: 10.12688/wellcomeopenres.21450.2. eCollection 2024. Wellcome Open Res. 2024. PMID: 39386968 Free PMC article.
-
Cryptococcal meningitis.Nat Rev Dis Primers. 2023 Nov 9;9(1):62. doi: 10.1038/s41572-023-00472-z. Nat Rev Dis Primers. 2023. PMID: 37945681 Review.
-
Treatment for HIV-associated cryptococcal meningitis.Cochrane Database Syst Rev. 2018 Jul 25;7(7):CD005647. doi: 10.1002/14651858.CD005647.pub3. Cochrane Database Syst Rev. 2018. PMID: 30045416 Free PMC article.
References
-
- Cohen DB, Zijlstra EE, Mukaka M, et al. Diagnosis of cryptococcal and tuberculous meningitis in a resource-limited African setting. Trop Med Int Health. 2010;15:910–7. - PubMed
-
- Castelnuovo B, Manabe YC, Kiragga A, et al. Cause-specific mortality and the contribution of immune reconstitution inflammatory syndrome in the first 3 years after antiretroviral therapy initiation in an urban African cohort. Clin Infect Dis. 2009;49:965–72. - PubMed
-
- Park BJ, Wannemuehler KA, Marston BJ, et al. Estimation of the current global burden of cryptococcal meningitis among persons living with HIV/AIDS. AIDS. 2009;23:525–30. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
