

A Clinical Scoring Algorithm for Determination of the Risk of Tuberculosis in HIV-Infected Adults: A Cohort Study Performed at Ethiopian Health Centers
- PMID: 25734163
- PMCID: PMC4324227
- DOI: 10.1093/ofid/ofu095
A Clinical Scoring Algorithm for Determination of the Risk of Tuberculosis in HIV-Infected Adults: A Cohort Study Performed at Ethiopian Health Centers
Abstract
Background: The World Health Organization (WHO) tuberculosis (TB) symptom screening instrument (WHO-TB) can identify human immunodeficiency virus (HIV)-infected individuals at low risk of tuberculosis (TB); however, many patients report WHO-TB symptoms and require further TB investigations. We hypothesized that further clinical scoring could classify subjects with a positive WHO-TB screening result (WHO-TB(+)) for the likelihood of TB.
Methods: HIV-infected adults eligible to initiate antiretroviral therapy (ART) were recruited and prospectively followed at 5 Ethiopian health centers. Irrespective of symptoms, all participants underwent sputum bacteriological testing for TB. Symptoms, physical findings, hemoglobin, and CD4 cell count results were compared between subjects with and those without bacteriologically confirmed TB. Variables associated with TB in WHO-TB(+) individuals were used to construct a scoring algorithm with multiple logistic regression analysis.
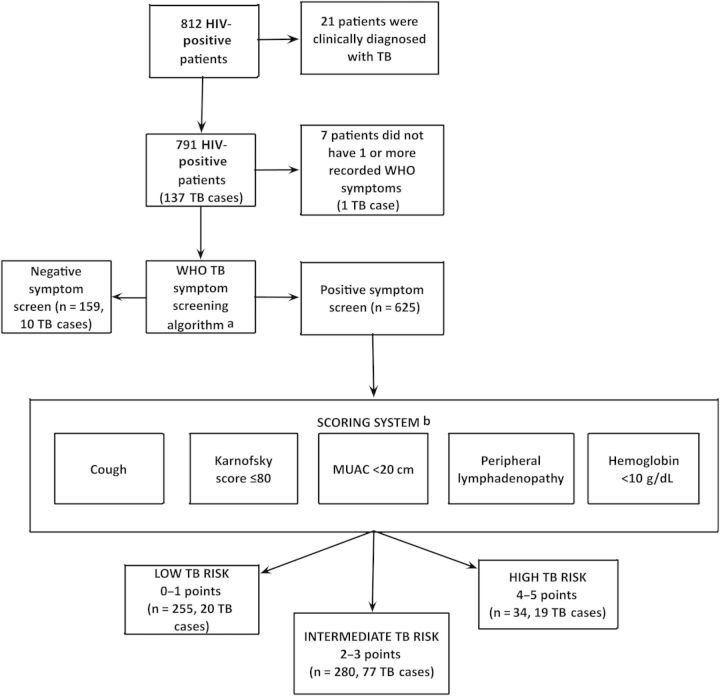
Results: Among 812 participants, 137 (16.9%) had TB. One hundred fifty-nine persons (20%) had a negative WHO-TB screen, 10 of whom had TB (negative predictive value [NPV], 94% [95% confidence interval {CI}, 90%-97.5%]). For WHO-TB(+) subjects, the following variables were independently associated with TB, and were assigned 1 point each in the clinical scoring algorithm: cough, Karnofsky score ≤80, mid-upper arm circumference <20 cm, lymphadenopathy, and hemoglobin <10 g/dL. Among subjects with 0-1 points, 20 of 255 had TB (NPV, 92% [95% CI, 89%-95%]), vs 19 of 34 participants with ≥4 points (positive predictive value, 56% [95% CI, 39%-73%]). The use of WHO-TB alone identified 159 of 784 (20%) with a low risk of TB, vs 414 of 784 (53%) using WHO-TB followed by clinical scoring (P< .001). The difference in proportions of confirmed TB in these subsets was nonsignificant (6.3% vs 7.2%; P= .69).
Conclusions: Clinical scoring can further classify HIV-infected adults with positive WHO-TB screen to assess the risk of TB, and would reduce the number of patients in need of further TB investigations before starting ART.
Clinical trials registration: NCT01433796.
Keywords: Ethiopia; HIV; health center; scoring; tuberculosis.
Figures
References
-
- World Health Organization. Geneva, Switzerland: WHO: 2013. Global tuberculosis report.
-
- Harries AD, Zachariah R, Corbett EL, et al. The HIV-associated tuberculosis epidemic—when will we act? Lancet. 2010;375:1906–19. - PubMed
-
- Getahun H, Harrington M, O'Brien R, et al. Diagnosis of smear-negative pulmonary tuberculosis in people with HIV infection or AIDS in resource-constrained settings: informing urgent policy changes. Lancet. 2007;369:2042–9. - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
